Remicade (infliximab) Inpatient and Outpatient Orders
advertisement
 Inpatient and Outpatient Orders")
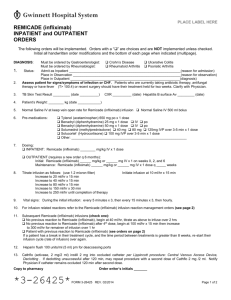
PLACE LABEL HERE REMICADE (infliximab) INPATIENT and OUTPATIENT ORDERS The following orders will be implemented. Orders with a “” are choices and are NOT implemented unless checked. Initial all handwritten order modifications and the bottom of each page when indicated (multipage). DIAGNOSIS: Must be ordered by Gastroenterologist: Crohn’s Disease Ulcerative Colitis Must be ordered by Rheumatologist: Rheumatoid Arthritis Psoriatic Arthritis 1. Admit as Inpatient __________________________________________(reason for admission) Place in Observation ________________________________________(reason for observation) Place in Outpatient __________________________________________(diagnosis) Status: 2. Assess patient for signs/symptoms of infection or CHF; notify MD if present prior to proceeding 3. TB Skin Test Result _________ (date __________) 4. Patient’s Weight: ________ kg (date ____________) 5. Normal Saline IV at keep vein open rate for Remicade (infliximab) infusion 6. Pre-medications: Tylenol (acetaminophen) 650 mg po x 1 dose Benadryl (diphenhydramine) 25 mg x 1 dose IV po Benadryl (diphenhydramine) 50 mg x 1 dose IV po Solumedrol (methylprednisolone) 40 mg 80 mg 125mg IVP over 3-5 min x 1 dose Other: _____________________________________________________________ 7. Dosing: INPATIENT: Remicade (infliximab) ________ mg/kg IV x 1 dose OUTPATIENT (requires a new order q 6 months): Initial: Remicade (infliximab) ______ mg/kg or ______ mg IV x 1 on weeks 0, 2, and 6 Maintenance: Remicade (infliximab) ______ mg/kg or ______ mg IV x 1 dose q _____ weeks Remicade (infliximab) doses within 25 mg of the nearest vial size may be rounded to that vial size 8. Titrate infusion as follows: (use 1.2 micron filter) Initiate infusion at 10 ml/hr x 15 min Increase to 20 ml/hr x 15 min Increase to 40 ml/hr x 15 min Increase to 80 ml/hr x 15 min Increase to 150 ml/hr x 30 min Increase to 250 ml/hr until completion of therapy 9. For infusion related reactions refer to the Remicade (infliximab) infusion reaction management orders (see page 2) 10. Subsequent Remicade (infliximab) infusions (check one): No previous reaction to Remicade (infliximab), begin at 40 ml/hr, titrate as above to infuse over 2 hrs No previous reaction to Remicade (infliximab) after 4th dose, begin at 100 ml/hr X 15 min then increase to 300 ml/hr for remainer of infusion over 1 hr Patient with previous reaction to Remicade (infliximab) (see orders on page 2) Send copy to pharmacy *3-26425* Order writer’s initials _______ FORM 3-26425 REV. 07/2012 Page 1 of 2 PLACE LABEL HERE REMICADE (infliximab) INPATIENT and OUTPATIENT ORDERS The following orders will be implemented. Orders with a “” are choices and are NOT implemented unless checked. Initial all handwritten order modifications and the bottom of each page when indicated (multipage). Prophylaxis for Subsequent Remicade (infliximab) Infusion Determined by previous reaction (Mild, Moderate, Severe) Mild Moderate 1. Pretreat with: 1. Pretreat with: a. Benadryl a. Benadryl (diphenhydramine) (diphenhydramine) 50 mg po x 1 dose 25 mg po x 1 dose b. Tylenol (acetaminophen) b. Tylenol (acetaminophen) 650 mg po x 1 dose 650 mg po x 1 dose c. Solu-Medrol (methylprednisolone) 2. Infuse Remicade (infliximab) 125 mg IVP x 1 dose over at least 2 hrs as 2. Remicade (infliximab) 1 mg test dose tolerated after pre-medications, wait 20 min 3. Infuse over at least 3 hrs as tolerated Severe 1. Physician present at administration 2. Pretreat with: a. Benadryl (diphenhydramine) 50 mg IV x 1 dose b. Tylenol (acetaminophen) 650 mg po x 1 dose c. Solu-Medrol (methylprednisolone) 125 mg IVP x 1 dose 3. Give Remicade (infliximab) 1 mg test dose after pre-medications, wait 20 min 4. Infuse over at least 4 hrs as tolerated Reaction Management Orders for Remicade (infliximab) Infusion Determine reaction type based on below, then follow mild, moderate or severe treatment orders Mild: 1. Pruritis or rash 2. Lightheadedness with < 20 point drop in systolic bp 3. Chest tightness without dyspnea/ wheezing 4. Headache 5. Shortness of breath 6. Warmth without temperature elevation 7. Flushing with no throat tightness Treatment of mild reaction: 1. Slow Remicade (infliximab) infusion rate to KVO 2. Benadryl (diphenhyramine) 25 mg po x 1 dose 3. Tylenol (acetaminophen) 650 mg po x 1 dose 4. Monitor vital signs q 10 min 5. Increase infusion rate as tolerated when patient is stabilized ______________ Date Moderate 1. Pruritis and/or rash 2. Hives without respiratory difficulty 3. Wheezing without dyspnea 4. Hypertension or hypotension with greater than 20 point but less than 40 point drop or rise in systolic blood pressure 5. Elevated temperature with rigors Severe (Notify Physician): 1. Dyspnea with wheezing 2. Dyspnea requiring ventilator support 3. Cardiopulmonary symptoms and urticaria 4. Hypotension with greater than 40 point drop in systolic blood pressure 5. Stridor (call for emergency support) Treatment of moderate reaction: Treatment of severe reaction (Notify Physician) 1. Pause Remicade (infliximab) infusion 1. Stop Remicade (infliximab) infusion 2. Benadryl (diphenhyramine) 50 mg IVP 2. Maintain NS at 100 ml/hr IV x 1 dose 3. Benadryl (diphenhyramine) 50 mg IVP x 1 3. Tylenol (acetaminophen) 650 mg po dose x 1 dose 4. Tylenol (acetaminophen) 650 mg po x 1 4. If wheezing present: dose Solu-Medrol (methylprednisolone) 5. Solu-Medrol (methylprednisolone) 125 mg IVP x 1 dose 5. 6. 125 mg IVP x 1 dose Monitor vital signs q 10 min 6. Restart infusion slowly after symptoms 7. resolve and vital signs are stable _______________ Time Monitor vital signs q 10 min Epinephrine (1:1000) 0.1 ml – 0.5 ml subcutaneous prn; may repeat q 5 min x 3 doses 8. Call for emergency support 9. Start oxygen to keep saturation > 90% 10. Physician to determine if transfer/admission is needed. _________________________________ Physician Signature ___________ PID Number Send copy to pharmacy FORM 3-26425 REV. 07/2012 Page 2 of 2