HYPERTENSIVE DISEASE IN PREGNANCY OBSTETRICS
advertisement

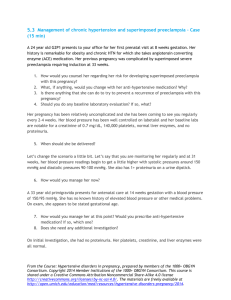
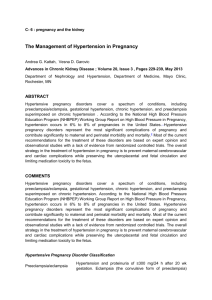
YL6 Pathologic OB SubModule [Obstetrics] OUTLINE I. Epidemiology II. Definitions & Modifications III. Clinical Types A. Gestational Hypertension B. Preeclampsia/Eclampsia C. Chronic Hypertension D. Chronic Hypertension with superimposed Preeclampsia/Eclampsia IV. Pathophysiology A. Preeclampsia B. Angiogenetic Factors of Preeclampsia C. Preeclampsia Physiology V. Clinical Approach A. Prediction B. Prevention C. Management of Eclampsia & Severe Preeclampsia I. II. 06 January 2011 HYPERTENSIVE DISEASE IN PREGNANCY EPIDEMIOLOGY 43.1 per 100 Pregnancies Pregnancy Induced Hypertension is the major cause of maternal mortality in England and Wales 18.42% of maternal deaths were due to PIH 56% of PIH due to eclampsia 2nd Most common medical complication encountered in pregnancy in the Philippines It is one of the most common causes of maternal mortality and an important cause of perinatal mortality and morbidity Dr. Sumpaico Keep in mind other factors that may increase blood pressure: Arm circumference, type of apparatus, time of BP measurement, “white-coat” HPN III. CLINICAL TYPES A. Gestational Hypertension 1. HTN without proteinuria occurring after 20 weeks gestation or postpartum. 2. It is a temporary diagnosis during pregnancy which has to be confirmed 12 weeks after delivery. o If BP becomes normal after 12 weeks, the final diagnosis is transient hypertension o If hypertension persists, the final diagnosis is chronic hypertension. B. Preeclampsia/Eclampsia 1. Preeclampsia The development of hypertension plus proteinuria, induced by pregnancy after the 20th week of gestation and sometimes earlier in extensive hydatidiform changes in chorionic villi. DEFINITIONS AND MODIFICATIONS Hypertension Systolic blood pressure (SBP) of at least 140 mmHg OR Diastolic blood pressure (DBP) of at least 90 mmHg Must be manifest on at least 2 occasions taken 6 hours apart Proteinuria Present when 300mg/liter/24 hour collection of urine is found; OR More than 1000mg/L/random sample in at least 2 random samples taken 6 hours apart Qualitatively, dipstick values of traces to 1+ signify mild while 2+ to 4+ signify heavy proteinuria Edema After 12 hours of bed rest, the presence of 1 – pitting edema; or a weight gain of 5 lbs or more/week Modifications in Classification and Definition Eliminate edema as a criterion for diagnosing preeclampsia As a diagnostic criterion for hypertension, the use of increased of 30 mmHg systolic or 15 mmHg diastolic above baseline is no longer recommended since they are not proven to be good prognostic indicators of outcome. Use Korotkoff phase V (disappearance of sound) for determination of diastolic pressure. Group ## INSERT. NAMES. OF. ALL. GROUP. MEMBERS. IN. ALPHABETICAL. ORDER. Criterion for severe preeclampsia 1. SBP ≥ 160 2. DBP ≥ 110 3. Proteinuria o ≥ 4 grams per day o ≥ +2 on dipstick 4. Oliguria <400 cc/day due to decreased RBF and GFR 5. Severe Headache or Visual Disturbance o (+) cerebral edema 6. Pulmonary Edema or cyanosis o Hemodynamic changes: increased afterload 7. Intrauterine Growth Restriction (IUGR) o decreased uteroplacental blood flow 8. RUQ or epigastric pain o Due to abnormal distension of Glisson’s capsule of the liver 9. Hemolysis Page 1 of 6 HYPERTENSIVE DISEASE IN PREGNANCY OBSTETRICS (endothelial dysfunction) diverse symptoms of preeclampsia and eclampsia o Manifests as increased serum LDH or hemoglobunuria 10. Elevated Liver Enzymes o Hepatocellular necrosis 11. Low Platelet Count o ≤ 100,000/mm3 (NV: 150,000/ mm3) o Microangiopathic hemolysis Picture of the diameter of spiral arteries in normal and abnormal arteries Current classification based on Age of Gestation: Early-onset preeclampsia Signs and symptoms < 34 weeks Late-onset preeclampsia Signs and symptoms ≥ 34 weeks AOG 2. Pregnant rats exposed to sFlt-1 had distinct clinical and pathological signs of preeclampsia, including the characteristics glomerular endotheliosis demonstrating for the first time a clear cause and effect between this protein and this disease Picture of preeclamptic arteries with proteinacious material (slfit1) Eclampsia The occurrence of convulsions, not caused by coincidental neurologic disease in a woman previously fulfilling the criteria for preeclampsia C. Chronic Hypertension BP ≥ 140/90 prior to pregnancy or before 20 weeks AOG and persists after 12 weeks postpartum OR Hypertension first diagnosed before 20 weeks gestation and persistent after 12 weeks postpartum D. Chronic HPN with Superimposed Preeclampsia/Eclampsia Pre-existing Chronic hypertension with new onset proteinuria and signs and symptoms of various endorgan dysfunction IV. PATHOPHYSIOLOGY Graph A ETIOLOGY OF HYPERTENSIVE DISEASE IN PREGNANCY (APPENDIX) Graph B Pro-angiogenetic factors vs. Anti-angiogenetic Placental GF, VEGF sFlt-1, Endoglin (dilators) (constrictors) If Pro-angiogenesis < Anti-angiogenesis = preeclampsia. On the other hand If Pro-angiogenesis > Anti-angiogenesis = Normal pregnancy SEE PICTURE IN OLD TRANS (CAN’T SEEM TO PASTE IT HERE) In vivo evidence Sflt-1 neutralizes effect of VEGF and PIGF and the loss of these GF damages the mother’s small blood vessels Group01 Rizzy. Ner. Berna. Mon. Dan. Bry. Page 2 of 6 HYPERTENSIVE DISEASE IN PREGNANCY OBSTETRICS Therefore, preeclampsia = high sFlt-1 and low PIGF Angiogenic Markers and the Risk for Pre-eclampsia Compairson of SFlt-1 among normotensive and hypertensive pregnancies PlGF clear difference There should be a drop of PlGF after 48 hours A. Preeclampsia Physiology Normal pregnancy: trophoblast invasion loss of tunica media elasticity decreased resistance, vasodilatation and increased perfusion Vascular system in normal pregnancy: Prostacyclin (endothelium-derived vasodilator)> Thromboxane (platelet-derived vasoconstrictor) Pre-eclampsia is the opposite of above The normal functional balance between vasoconstriction and vasodilation eicosanoids is disturbed in preeclampsia B. V. CLINICAL APPROACH Leon Chesley: “Radical therapies: mastectomy, oophorectomry, renal decapsulation, trephnation, alighment of the patient with the earth’s magnetic fields” have been employed as treatments for preeclampsia in the past A. Prediction WHO Criteria for a Screening Test a. Is there a significant burden? b. Is there a preclinical (asymptomatic stage)? c. Will detection improve outcomes? d. Is the screening test cost-effective accurate and acceptable to patients? e. Is there an effective treatment available for detected disease? Group01 Patient Profile: o Primigravida o Poor o Young o Non-white o Protein intake suboptional o Prenatal checks: late or none o Family history of hypertension o Low SES Risk Factors Associated with Pregnant Woman: o High BMI is now a risk factor Risk Factors Associated with Husband: Rizzy. Ner. Berna. Mon. Dan. Bry. o First time father o Previously fathered a pre-eclamptic Associated with Fetus: o Multifetal pregnancy o Hydrops/triploidy o Hydatidiform mole Physical Examination Blood Pressure Mean Arterial Pressure o MAP = DBP + 1/3 (SBP-DBP) o MAP-2 >90 mmhg OR MAP-3 >105 mmhg associated with increased PIH and perinatal deaths o Absence of a mid trimester drop in blood pressure may predict future PIH based on the absence of arteriolar vasodilation Roll Over Test (ROT) o No longer used Combined MAP-2 and ROT o Performed singly the MAP-2 or the ROT predicted >60% of those at risk of PIH o Combining the MAP-2 and ROT predicted >78% of those at risk of PIH Uterine Artery Doppler o Doppler ultrasound in high-risk pregnancy (especially those with hypertension and IUGR) were associated with reduction in perinatal deaths (OR 0.71, 0.50 to 1.01) Doppler Velocimetry o Meta analysis of RCTs in high risk pregnancies showed significant reduction in antennal admission, labor induction, CS, fetal death and distress Placental volume o 3D technology o 1st trimester o Identify future IUGR and preeclampsia Quad test markers in Down Syndrome screening o AFP, B-HCG, Ue3, Inhibin o Pappa a and B-HCG o VEGF, PIGF, SFLT1 o Endoglin o Pp13: 90% detection rate o Detection rate for combinations markers: 3444%: Uterine Doppler plus marker increase the sensitivity SUMMARY: Assess Risk Factors: assess right away in the first visit (1st visit) Measure blood pressure (1st visit) “Thin is in, stout is out” BMI/Obesity: counsel against obesity Use of diagnostic biochemical markers: available in the market PIGF, VEGF SLFT1, endoglin Pp13 Page 3 of 6 HYPERTENSIVE DISEASE IN PREGNANCY C. o High dose calcium exerts a negative feedback effect on parathyroid hormone lowering intracellular calcium ion levels smooth muscle relaxation and diminished responsiveness to pressor stimuli o You cut the risk of developing preeclampsia by 50% with calcium intake. There is a theoretical risk of developing renal calculi with high dose calcium but it has not been proven Calcium will diminish by half the risk of preeclampsia and reduce death or serious morbidity Use of Uterine Artery Doppler o Observe diastolic notches, resistance and pulsatility indices and placental volume Combination: most important is to screen during the middle of the pregnancy using Doppler and biochemical marker measurement At 17 weeks AOG, do biochemical tests At 22 weeks AOG, do Doppler tests Prevention 1. Bed Rest 2. Diuretics 3. Anti-platelets - low dose aspirin The normal functional balance between vasoconstriction and vasodilation eicosanoids is disturbed in preeclampsia Mechanism of action: the selective effect of ASA on eicosanoids is mainly attributable to the cell biologic differences between platelets and endothelium. Platelets are anucleated, while endothelium is nucleated and thus able to regenerate. Mechanism of action: Deactelyated in peripheral tissues make sure you use it only with high-risk patients. Aspirin may be given provided: o Patients have been identified as high-risk based on previous history of HPN, adverse obstetric outcomes, MAP or roll-over tests, abnormal Doppler waveforms or angiotensin sensitivity tests. o Patient has no history of aspirin allergy or hypersensitivity (Acid peptic disease or coagulopathy) o Treatment is started during the second trimester to prevent fetal malformations in the first trimester o Pediatric doses are kept at 60-80 mg/day based on majority of reports Make sure you monitor platelet and coagulation profile Monitor fetal ductus arteriosus and amniotic fluid volume by ultrasound No deleterious effect on the fetus and neonate as long as within pediatric dose of 60-80 mg/day. Antiplatelet trials have shown similar results. 4. OBSTETRICS High Dose Calcium Study of Guatemalan Indians: those who ate corn with calcium did not develop preeclampsia while those who ate only raw corn developed it. Prevention can be done by simply adding calcium to the diet. There is a 30% drop of BP with calcium and a drop in the incidence of preeclampsia o Oral intake of 2 grams per day has been proposed to prevent preeclampsia Rizzy. Ner. Berna. Mon. Dan. Bry. Nitric Oxide (NO) Donors AKA Endothelium-derived relaxing factor (EDRF) A byproduct of L-arginine metabolism and has a vasodilatory and mitogenic effect 6. Antioxidants Ex. Vitamins C and E Initial studies were done but current evidence now shows that it is not beneficial. 7. Anti-sFlt-1 The Chinese have now developed these as treatment through recombinant studies. 8. Recombinant VEGF/PLGF SUMMARY Low-dose Aspirin High-dose Calcium Anti-SFLT1 Recombinant VEGF and PIGF D. Management of Eclampsia and Severe Preeclampsia 1. Anti-convulsants Convulsion control with Magnesium Sulfate MgSO4 Halves the risk of pre-eclampsia and reduces the risk of maternal death Administered as follows A: Loading dose: 4 gm IV bolus over 5 minutes + Maintenance dose: 1 gm per hour IV drip B: Loading dose: 4 gm IV bolus slowly over 5 minutes and 10gm IM (5 gm into each buttock) followed by: Maintenance dose: 5 gm IM every 6 hours PRECAUTIONS: 1. The presence of deep tendon reflexes (DTRs) 2. Respiratory rate of >12 per minute 3. Urine output of at least 100 cc/4 hours Note: continue anti-convulsion therapy even 24 hours after the woman has delivered Different Magnesium Sulfate levels in the body Group01 5. Page 4 of 6 HYPERTENSIVE DISEASE IN PREGNANCY o o o o o Group01 OBSTETRICS 2 meqs – normal, tolerable 7 – 10 meqs – lose patellar reflex 12 meqs - prolonged AV condutccion 15 meqs - respiratory failure 24 meqs – cardiac arrest 2. Anti-Hypertensives Hydralazine – drug of choice Labetalol CA blockers (nifedipine, nicardipine) Alpha adrenergic blockers – Clonidine Low dose diazoxide Nitroprusside Do not give ACE inhibitors: can cause kidney problems and bone lesions in the neonate 3. Delivery 1) Age of gestation – once the 34 weeks of pregnancy is achieved, delivery is recommended for maternal safety 2) Severity of the disease Severe preeclampsia patients are usually delivered once 34 weeks of pregnancy is achieved but conservative measures at <34 weeks can be tried in high risk centers. Properly informed patients with mild preeclampsia can be managed from home. 3) Maternal evaluation Regular checks of the mother’s multipleorgan symptoms, vital signs, body weight, input & output monitoring and regular review of meaningful laboratory examinations are mandatory 4) Fetal status Fetus should be regularly monitored with daily fetal counts, non-stress test, contraction stress test, biophysical profile growth monitoring, Doppler, steroids have proven invaluable. 5) Nursery capability Most Philippine nurseries report a high survival rate at 34 weeks Rizzy. Ner. Berna. Mon. Dan. Bry. Page 5 of 6 HYPERTENSIVE DISEASE IN PREGNANCY Group01 Rizzy. Ner. Berna. Mon. Dan. Bry. OBSTETRICS Page 6 of 6