ชื่อเรื่องภาษาไทย (Angsana New 16 pt, bold)
advertisement
")
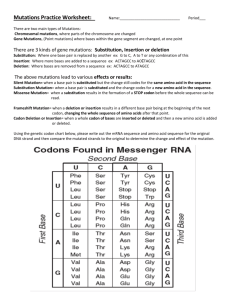
Frequency of K-ras Mutation in Endometrioid Endometrial Adenocarcinoma Papitchaya Watcharanuruk1*, Supaporn Suwiwat2, Siriwong Lattakanjanang3 1 Department of Biomedical Sciences, Faculty of medicine, Prince of Songkla University, Songkhla 90110, Thailand 2 Department of Pathology, Faculty of medicine, Prince of Songkla University, Songkhla 90110, Thailand *e-mail: papitchaya_59@hotmail.com Abstract K-ras oncogene plays an important role in the mechanism of carcinogenesis in many human cancers. Previous studies have shown that K-ras mutation is found in 10% to 30% of endometrial carcinomas. However, the K-ras mutations in Thai patients with endometrial carcinoma have not yet been investigated. Our purpose was to examine the frequency of Kras gene mutation in endometrioid adenocarcinoma and investigate the correlation with clinicpathological variables. Genomic DNA was extracted from formalin-fixed paraffinembedded tissue sections. Polymerase chain reaction amplification for K-ras codon 12 and 13 were performed, followed by sequencing. K-ras mutations were detected in 10 of 62 (16.1%) endometrioid adenocarcinomas. Six mutations were found at codon 12 (9.7%), and two mutations at codon 13 (3.2%). Interestingly, we also detected 2 samples with a double point mutations, codon 12 and codon 6 (1.6%), and codon 12 and codon 7 (1.6%). No significant relationship was seen between the presence of K-ras mutations and clinicopathological variables such as age, grade, and depth of myometrial invasion. Our findings suggest that mutation of K-ras gene may be associated with pathogenesis of endometrioid adenocarcinoma in subgroup patients but with no evidence of prognostic value. Keywords: K-ras mutation, endometrioid adenocarcinoma Introduction Endometrial carcinoma is the third common malignant tumor of the female genital system in Thailand with the incidence rate of 2.8/100,000/years [1]. Recently, the incidence in Thai women younger than 40 years of age who have obesity seems to be increasing [2, 3]. Endometrioid adenocarcinoma is the major type of endometrial carcinoma, approximately 80% of all cases. This type is commonly associated with high levels of estrogen. In addition, it is related to the history of obesity, diabetes, hypertension, nulliparity, and chronic anovulation [4, 5]. The pathogenensis of endometrioid adenocarcinoma also involves a wide range of molecular alterations, including microsatellite instability, PTEN mutation, K-ras (cKirsten-ras/ Kirsten Rat Sarcoma virus) mutation, and β-catenin mutation [6, 7]. K-ras is a proto-oncogene and it encodes a 21 kDa small monomeric guanine nucleotide-binding protein (G-protein). The G-protein has been implicated mainly in regulating cell growth and differentiation. Mutations of K-ras oncogene result in constitutive activation of the signal transduction pathway and subsequently upregulated proliferation and impaired differentiation [8]. Previously published studies have shown that K-ras gene mutation is found in 10% to 30% of endometrial carcinomas [9, 11-14]. K-ras mutation has been reported in association with submicroscopic myometrial invasion and depth of myometrial invasion in endometrial cancer [10]. In addition, K-ras mutations have been identified in endometrial hyperplasia and complex atypical hyperplasia, suggesting that K-ras mutation may be an early event in the carcinogenesis of endometrium [11, 12]. However, Kras mutations in uterine adenocarcinoma in Thai patients have not yet been investigated. In this study, we examine the frequency of K-ras mutations in Thai patients with endometrioid adenocarcinoma and investigate the correlation between the presence of K-ras mutations and clinicopathogical variables including age, grade, and depth of myometrial invasion. Methodology Patients and tissue samples Formaldehyde-fixed, paraffin-embedded tissue from cases of endometrioid adenocarcinoma of the uterus were collected for this study. The samples were obtained from 62 cases treated at Songklanagarind University Hospital during 2011-2012, including hysterectomy specimens in all cases. This study was approved by the Hospital Ethics Committee. DNA extraction and PCR analysis DNA was extracted from 5-μm from paraffin section using QIAamp Tissue Kit (Qiagen) following the manufacturer’s protocol. The PCR for K-ras exon2 was performed using primer K-ras forward: 5’-GGTACTGGTGGAGTATTTGAT-3’, and K-ras reverse:5’ACTCATGAAAATGGTCAG AG-3’. To determine that all samples originally contained DNA of sufficient quality and quantity, samples were co-amplified for the presence of an internal standard, beta globin. The beta-globin primer were PC04:5’-CAACTTCATCCACG TTCACC-3’, and GH20:5’-GAAGAGCCAAGGACAGGTAC-3’. The amplification reaction was performed with initial denaturation at 94oC for 4 min, followed by 40 cycles of denaturation 94oC for 45 sec, annealing at 51 oC (K-ras), 55 oC (beta-globin) for 45 sec, and extension at 72 oC for 1 min, and with final extension at 72 oC for 7 min. The 291 bp of K-ras product and the 268 bp of beta-globin product were run on a 2% agarose gel electrophoresis and stained with ethidium bromide for size verification. Direct sequencing The PCR products were purified using Purelink PCR Purification kit (Invitrogen) according to the manufacturer’s instruction. The purified PCR products were use as template in cycle sequencing with the Big Dye Terminator v1.1 kit (Applied Biosystem). The sequencing reactions were ethanol precipitated and run on a ABI PRISM 310 DNA sequencer (Applied Biosystem). Statistical analysis The relationship between K-ras mutation and clinicopathological variables was determined using Fisher’s Exact test. Statistical significance was set at P < 0.05. Results K-ras mutations were analyzed in 62 endometrioid adenocarcinomas and the incidence of K-ras mutations was 16.1% (10 of 62, Table1). Of the 10 mutations, 60% (6 of 10) were found in codon 12, 20% (2 of 10) in codon 13, and 20% (2 of 10) in codon 12 with codon 6 and codon 12 with codon 7, subsequently. No significant relationship was seen between the presence of K-ras point mutation and clinicopathological variables, including age, grade, and depth of myometrial invasion as shown in Table 2. Table 1. Type of K-ras point mutations and amino acid change Mutation Hotspot codon mutations codon 12 Nucleotide change Amino acid change K-ras mutation GGT > TGT GGT > GAT GGT > AGT GGT > GTT Gly12Cys (G12C) Gly12Asp (G12D) Gly12Ser (G12S) Gly12Val (G12V) 2 2 1 1 GGC > TGC GGC > GAC Gly13Cys (G12C) Gly13Asp (G12D) 1 1 GGT > TGT TTT > CTT Gly12Cys (G12C) Phe6Leu (F6L) codon 13 codon 12 and codon 6 1 codon 12 and codon 7 1 GGT > GAT GTG > ATG Gly12Asp (G12D) Val7Met (V7M) Table 2. Clinicopathologic variables related to presence of K-ras mutation. Data Total Age (years) <50 50-60 >60 Number of cases 62 Cases of K-ras mutation 10 p value 12 31 19 3 5 2 NS Histological grade G1 G2 G3 33 16 13 6 3 1 NS Myometrial invasion (%) none <50% ≥50% 5 32 25 0 6 4 NS NS= No Significant Discussion and Conclusion The results from this study show that 16.1% (10 of 62) endometrioid adenocarcinomas demonstrated K-ras mutations. The frequency of K-ras mutation in endometrioid adenocarcinomas in our study is similar to other published reports, ranging from 10% to 30% [11-14]. K-ras mutational analysis in this study revealed that each affected case contained a single point mutation, either within codons 12 (G12C, G12D, G12S, and G12V) or 13 (G13C and G13D). These data types of K-ras gene mutations are consistent with the previous reports [15]. Most of the K-ras mutations found in human tumors involve these codon 12 and 13, coding for glycines located in proximity of the catalytic site of RAS. Any mutation resulting in the incorporation of a different amino acid at these positions leads to a reduction of the intrinsic GTPase activity of RAS [16]. It is interesting that our data showed a double point mutation of K-ras mutation (2 of 62) at codon 12 and 6 (G12C, F6L), and codon 12 and 7 (G12D, V7M). In summary, our findings demonstrate the contributions of K-ras mutation both a single point mutation within codon 12 or 13 and a double point mutation to pathogenesis of endometrioid adenocarcinoma and indicate no correlation with clinicopathological variables such as age, grade, and depth of myometrial invasion. References 1. Khuhaprema T, Srivatanakul P, Sriplung H, Wiangnon S, Sumitsawan Y, Attasara P, editors. Cancer in Thailand Vol.V 2001-2003. Bangkok 2010. 2. Hanprasertpong J, Sakoprakraikij S, Geater A. Endometrial cancer in Thai women aged 45 years or younger. Asian Pac J Can Prev. 2008; 9:58-62. 3. Manchana T, Khemapech N. Endometrial Adenocarcinoma in Young Thai Women. Asia Pacific J Cancer Prev. 2008; 9:283-6. 4. Dahlgren E, Friberg LG, Johansson S, Lindström B, Odén A, Samsioe G, et al. Endometrial carcinoma; ovarian dysfunction—a risk factor in young women. Eur J Obstet Gynecol Reprod Biol. 1991; 41:143-50 5. Doll A, Abala M, Rigaua M, Monge M, Gonzaleza M, Demajoa S, et al. Novel molecular profiles of endometrial cancer-new light through old windows. J Steroid Biochem Mol Biol. 2008; 108:221-9. 6. Soliman PT, Oh JC, Schmeler KM, Sun CC, Slomovitz BM, Gershenson DM, et al. Risk factors for young premenopausal women with endometrial cancer. Obstet Gynecol. 2005; 105:575-80. 7. Bansal N, Yendluri V, Wenham RM. The molecular biology of endometrial cancer and the implications for pathogenesis, classification, and targeted therapies. Cancer Control. 2009; 16:8-13. 8. Kiaris H, Spandidos D. Mutations of ras genes in human tumors (review). Int J Oncol. 1995; 7:413-21. 9. Lax SF. Molecular genetic pathways in various types of endometrial carcinoma: from a phenotypical to a molecular-based classification. Virchows Archiv. 2004; 444:213-223. 10. Alexander-Sefre F, Salvesen HB, Ryan A, Singh N, Akslen LA, MacDonald N, et al. Molecular assessment 11. 12. 13. 14. 15. 16. of depth of myometrial invasion in stage I endometrial cancer: a model based on K-ras mutation analysis. Gynecol Oncol. 2003; 91:218-25. Sasaki H, Nishii H, Takahashi H, Tada A, Furusato M, Terashima Y, et al. Mutation of the Ki-ras protooncogene in human endometrial hyperplasia and carcinoma. Cancer Res. 1993; 53:1906-10. Dobrzycka B, Terlikowski SJ, Mazurek A, Kowalczuk O, Niklińska W, Chyczewski L, et al. Mutations of the KRAS oncogene in endometrial hyperplasia and carcinoma. Folia Histochem Cytobiol. 2009; 41:14350. Duggan BD, Felix JC, Muderspach LI, Tsao JL, Shibata DK. Early mutational activation of the c-Ki-ras oncogene in endometrial carcinoma. Cancer Res. 1994; 54:1604-7. Lax S, Kendall B, Tashiro H, Slebos RJ, Hedrick L. The frequency of p53, K-ras mutations, and microsatellite instability differs in uterine endometrioid and serous carcinoma: evidence of distinct molecular genetic pathways. Cancer. 2000; 88:814-24. Xiong J, He M, Jackson C, Ou JJ, Sung CJ, Breese V, et al. Endometrial carcinomas with significant mucinous differentiation associated with higher frequency of K-ras mutations: A morphologic and molecular correlation study. Int J Gynecol Cancer. 2013; 23:1231-6. Scheffzek K, Ahmadian M, Wittinghofer A. GTPase-activating proteins: helping hands to complement an active site. Trends Biochem Sci. 1998; 23:257-62. Acknowledgements: This work was supported by a grant from faculty of medicine, Prince of Songkla University.