AAP Adult Symptom Checklist
advertisement

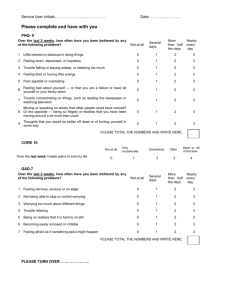
AAP ADULT SYMPTOM CHECKLIST A. During the last 4 weeks, how much have you been bothered by any of the following problems? 1= Never 2 =Some days 3 = More than half the days 4 =Nearly daily _____1. Stomach pain. _____2. Back pain _____3. Pain in your arms, legs, or joints (knees, hips, etc.) _____4. Feeling tired or having little energy _____5. Trouble falling or staying asleep, or sleeping too much _____6. Menstrual cramps or other problems with your periods _____7. Pain or problems during sexual intercourse _____8. Headaches _____9. Chest pain ____10. Dizziness ____11. Fainting spells ____12. Feeling your heart pound or race ____13. Shortness of breath ____14. Constipation, loose bowels, or diarrhea ____15. Nausea, gas, or indigestion B. Over the last 2 weeks, how often have you been bothered by any of the following problems? 1= Never 2 =Some days 3 = More than half the days 4 =Nearly daily _____1. Feeling nervous anxiety or on edge _____2. Not being able to stop or control worrying _____3. Worrying too much about different things _____4. Trouble relaxing _____5. Being so restless that it is hard to sit still _____6. Becoming easily annoyed or irritable _____7. Fearing something awful might happen C. Questions about anxiety attacks. NO YES a. In the last 4 weeks, have you had an anxiety attack ⎯ suddenly fear or panic? NO YES b. Has this ever happened before? NO YES c. Do some of these attacks come suddenly out of the blue ⎯ that is, in situations where you don’t expect to be nervous or uncomfortable? NO YES d. Do the attacks bother you a lot or are you worried about having another attack? NO YES e. During your last bad anxiety attack, did you have symptoms like shortness of breath, sweating, or your heart racing, pounding or skipping? D. Over the last 4 weeks, how often have you been bothered by any of the following problems? 1= Never 2 =Some days 3 = More than half the days 4 =Nearly daily _____a. Feeling nervous, on edge, or worrying a lot _____b. Feeling restless so that it is hard to sit still. _____c. Getting tired very easily. _____d. Muscle tension, aches, or soreness. _____e. Trouble falling asleep or staying asleep. _____f. Trouble concentrating on things. _____g. Becoming easily annoyed or irritable. _____h. Feeling emotionally numb or disconnected E. Have you used alcohol in the past 12 months (includes beer and wine)? NO___ YES____ _____1. How often do you consume alcohol? 1=Never 2= Once a week, 3= 2-4 times per week 4=Nearly daily 2. Have you ever had a DWI, PI, MIP, or other legal problem with alcohol? NO___ YES____ 3. In the past 2 weeks how many have you had: ____beer ___glasses of wine ____shots/cocktails F. Over the last 2 weeks, how often have you been bothered by any of the following problems? 1= Never 2 =Some days 3 = More than half the days 4 =Nearly daily _____1. Little interest or pleasure in doing things _____2. Feeling down, depressed, or Hopeless _____3. Trouble falling/staying asleep, or sleeping too much _____4. Feeling tired or having little energy. _____5. Poor appetite or overeating. _____6. Feeling bad about yourself — that you are a failure or have let yourself or your family down. _____7. Trouble concentrating on things, such as reading the newspaper or watching television _____8. Moving or speaking so slowly that other people could have noticed? Or the opposite – being so fidgety or restless that you have been moving around a lot more than usual. _____9. Thoughts that you would be better off dead of or hurting yourself in some way ____10. Excessive tearfulness G. If you checked off any problems on this questionnaire, how difficult have these problems made it for you to do your work, take care of things at home, or get along with other people? ___ Not difficult at all ___Somewhat difficult ___Very difficult ___ Extremely difficut If you are experiencing any of the problems on this form, how difficult have these problems made it for you to do your work, take care of things at home or get along with other people? ___ Not difficult at all Yes_____ Yes_____ Yes_____ ___Somewhat difficult ___Very difficult ___ Extremely difficut No_____Has there been a time in the past month when you have had serious thoughts about ending your life? No_____Have you EVER, in your WHOLE LIFE, tried to kill yourself or made a suicide attempt? No_____In the past three months, have you acted aggressively toward others? If you are having thoughts that you would be better off dead or of hurting yourself or someone else in some way, please discuss this with your Health Care Clinician, go to a hospital emergency room or call 911