Patient Reported Outcomes Assessment KDQOL What is the purpose of the study?
advertisement

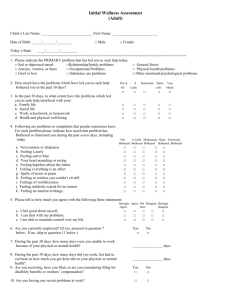
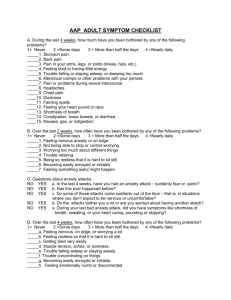
Patient Reported Outcomes Assessment KDQOL 35 Symptom List What is the purpose of the study? This part of the study is being carried out in cooperation with physicians and their patients. The purpose is to assess the quality of life and symptoms of patients with autonomous hyperparathyroidism. What will I be asked to do? For this study, we want you to complete a survey today about your health and how you feel. Please put an “X” in the box next to your answer to each question. Confidentiality of information? We do not ask for your name. Your answers will be combined with those of other participants in reporting the findings of the study. Any information that would permit identification of you will be regarded as strictly confidential. How will participation benefit me? The information you provide will tell us how you feel about your care and further understanding about the effects of medical care on the health of patients. This information will help to evaluate the care delivered to patients with autonomous hyperparathyroidism. Thank you for completing this survey! These questions are about how much you were bothered by certain conditions during the past 4 weeks. For each question, please give the one answer that comes closest to the way you have been feeling. 1. During the past 4 weeks, to what extent were you bothered by each of the following? [Mark one box on each line] Not at all Somewhat Moderately bothered bothered bothered Very Extremely much bothered bothered A Dry skin? .............................. 1 2 3 4 5 B Itchy skin? ............................ 1 2 3 4 5 C Lack of strength? ................. 1 2 3 4 5 D Fatigue, weakness? .............. 1 2 3 4 5 E Washed out or drained? ....... 1 2 3 4 5 F Muscle soreness? ................. 1 2 3 4 5 G Excessive thirst? .................. 1 2 3 4 5 H Dry mouth?........................... 1 2 3 4 5 I Joint pain? ............................ 1 2 3 4 5 J Trouble sleeping? ................. 1 2 3 4 5 K Easy bruising? ...................... 1 2 3 4 5 L Sleepiness during day? ........ 1 2 3 4 5 M Cramps during dialysis?....... 1 2 3 4 5 N Joint stiffness?...................... 1 2 3 4 5 O High blood pressure? ........... 1 2 3 4 5 P Back pain? ............................ 1 2 3 4 5 KDQOL-35-Symptom List - United States/English - Mapi Research Institute. f:\institut\cultadap\project\5356\study5356\questionnaire\original\forproject\kdqol-35-symptom list_ts1.0_eng-usori-for vf.doc-05/08/09-az Not at all Somewhat Moderately bothered bothered bothered Very Extremely much bothered bothered Numbness in hands or feet? ...................................... 1 2 3 4 5 R Bone aches? ......................... 1 2 3 4 5 S Muscle spasms? ................... 1 2 3 4 5 T Lack of appetite? .................. 1 2 3 4 5 U Headaches?........................... 1 2 3 4 5 V Nausea or upset stomach? ............................... 1 2 3 4 5 W Low blood pressure? ............ 1 2 3 4 5 X Trouble with memory? ......... 1 2 3 4 5 Y Shortness of breath? ............. 1 2 3 4 5 Z Cramps after dialysis? .......... 1 2 3 4 5 AA Faintness or dizziness? ........ 1 2 3 4 5 BB Hot or cold spells? ............... 1 2 3 4 5 CC Trouble concentrating? ........ 1 2 3 4 5 DD Trouble getting breath? ........ 1 2 3 4 5 EE Blurred vision? ..................... 1 2 3 4 5 FF Chest pain? ........................... 1 2 3 4 5 GG Swelling of ankles? .............. 1 2 3 4 5 HH Loss of taste?........................ 1 2 3 4 5 II Clotting or other access site problems? ...................... 1 2 3 4 5 Q KDQOL-35-Symptom List - United States/English - Mapi Research Institute. f:\institut\cultadap\project\5356\study5356\questionnaire\original\forproject\kdqol-35-symptom list_ts1.0_eng-usori-for vf.doc-05/08/09-az