Medical Questionnaire
advertisement

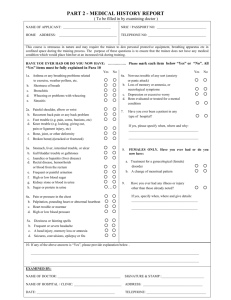
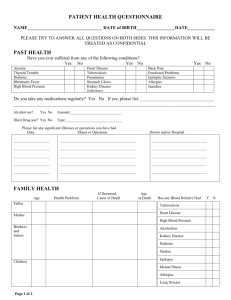
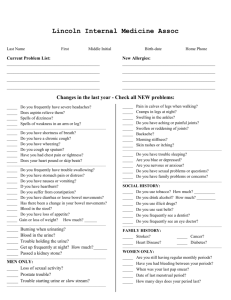
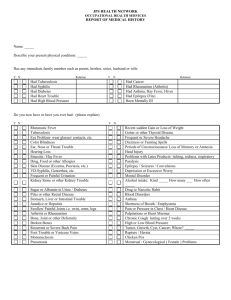
RIVERSIDE GROUP (LONDON) Ltd Medical Questionnaire Name: _______________________________ Please complete the following form to confirm your current & past medical history. We ask you to complete this for your own safety and that of others who you may be working with. Please be as honest as you can. The information that you provide to us is private and confidential. How would you describe your current state of health? (Delete as appropriate) POOR / AVERAGE / GOOD / EXCELLENT Are you currently suffering from any medical condition that prevents you from undertaking any type of employment? If yes, please specify. Are you currently on any medication? If yes, what for? How many days off sick have you had in the last year? Have you had an operation? If yes, what for? If you answered yes to number 5, have you made a full recovery or does it still affect you? Are you currently or have you ever been registered disabled? Please put tick next any of the following that you have ever suffered from or are currently affected by. Allergies Asthma Back Trouble Bowel Trouble Diabetes Chest Trouble Dysentery Ear Trouble Epilepsy Eye Trouble Fainting or blackouts Hay fever Heart Trouble Hepatitis B High Blood Pressure Recurring Head Aches Mental Illness Salmonella Skin Trouble Stomach Trouble Tuberculosis Typhoid Fever Varicose Veins Fear Of Heights Thank you for taking the time to complete the above questions. Please sign below to confirm that all information that you have given above is correct. Should Riverside Group ( London ) Ltd feel the need to clarify any information that you have given; your signature at the bottom of this page is your authorisation for us to do so with your GP. We will approach you for these details when required. Signature: _______________________ Date: ___________________________