Pulmonary Pathophysiology Chart
advertisement

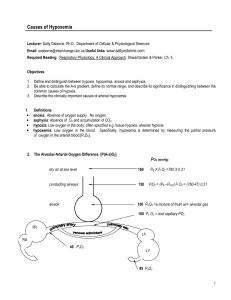
Pathophysiology Symptoms Asthma Hypersensitivity, responds to environmental triggersAfferent nerve stimulation Parasympathetic Immune Response affecting Airways REVERSIBLE Parasympathetic: Cough (clear mucus) Vasodilation, Bronchoconstriction (smooth muscle hypertrophy in extreme cases) BM thickening Mucosal secretions Dyspnea Breath Sounds: Wheezing, Tachypnea (as a compensation for hypoxemia) Tachycardia (vasodilation due to low pO2, leads to compensatory increase in CO due to decreased TPR) Pulsus Paradoxus Chronic Bronchitis Does not respond to environmental triggers (except asthmatic bronchitis) Comes from acute bronchitis (like asthma) Afferent Nerve Stimulation Parasympathetic Immune Response affecting Airways Parasympathetic: Productive Cough Vasodilation, Bronchoconstriction (smooth muscle hypertrophy) BM thickening Mucosal secretions Emphysema Destruction of 1.) terminal respiratory units and 2.) alveolar capillary beds 3.) elastic tissue Protease Inhibitor DeficiencyElastolytic Activity Dyspnea Breath Sounds: Wheezing, Coarse Crackles Long Slow Breathing Dyspnea Breath Sounds: Wheezing, Crackles, Rales Tachypnea (as compensatory for hypoxemia) Tachycardia (vasodilation due to low pO2, leads to compensatory increase in CO due to decreased TPR) Polycythemia (due to Chronic Hypoxemia) Jugular Vein Distention due to Pulmonary HPTN (due to Chronic Hypoxemia) may lead to Cor Pulmonale Tachycardia (vasodilation due to low pO2, leads to compensatory increase in CO due to decreased TPR) Polycythemia (due to Chronic Hypoxemia) Jugular Vein Distention due to Pulmonary HPTN (due to Chronic Hypoxemia) May lead to Cor Pulmonale Cough is rare V/Q Ratios Pulmonary Tests Compliance Inflammation Hypoxemia Hypocapnia Hypercapnia High V/Q and Low V/Q: Because of non-homogenous airway obstruction, we have overventilated non-obstructed respiratory units (High V/Q, due to tachypnea) and we have underventilated obstructed units (low V/Q). ↓FEV1/FVC ↓Compliance due to Hyperinflation of Lungs Yes Yes Yes, due to compensatory increase in respiratory ratehyperventilation of nonobstructed respiratory units. Yes, severe asthma attack Low V/Q only, (no compensatory tachypnea): Increase in Physiological Shunting. High V/Q only, (destruction of alveolar capillary beds): Increase in Physiological Dead Space. ↓FEV1/FVC ↓Compliance due to Hyperinflation of the Lungs Yes Yes, Chronic No ↓FEV1/FEV ↑Compliance due to Alveolar Wall Degeneration No Yes, Chronic No, because even though we have tachypnea, the damage is homogenous and all units are obstructed. Yes Yes, this attempts to increase RR IPF (Idiopathic Pulmonary Fibrosis-idiopathic means no one knows etiology) Type I Epithelial Cell Destruction, replacement by abnormal Type II Proliferating Type Cells Scarring and Inflammation in Alveolar Units ↓in Surfactant (↓Compliance ↑Lung Recoil via ↑elastic recoil and ↑surface tension) Thickening of Alveolar-Capillary Membrane, Loss of Capillary Beds Symptoms Idiopathic Symptoms: Dry Nonproductive Cough Dyspnea Tachypnea (due hypoxia, and increased respiratory drive due to stimulation of the C fibers/J receptors in the alveolar walls) Inspiratory Crackles (due to fibrosis and loss of normal surfactant) Digital Clubbing JVD from Pulmonary HPTN (which is a result of hypoxemia and capillary bed destruction-capillary bed destruction makes it difficult to flow through those regions) Cor Pulmonale V/Q Ratios High V/Q (due to thickening of Alveolar-Capillary Membrane and Loss of Capillary Beds via Scarring and Inflammation) Low V/Q (due to ↓compliance) Pulmonary Tests FEV1/FVC same (because of proportionate decrease in both FEV1 and FVC) Compliance ↓ Inflammation Yes Hypoxemia Yes, Chronic Hypocapnia Yes, sometimes (mild hypocapnia due to tachypnea) Hypercapnia Yes, in the later stages of the disease when the increased work of breathing prevents ventilation Question: How does hypoxemia occur in the presence of hypocapnia? I thought they both take only 0.25 sec to exchange in the blood. Pathophysiology Answer: It is easier to get rid of CO2, because all it is doing is waiting to be eliminated. However, the O2 brought in needs to be used by the tissues and so full replenishment of O2 in the blood is difficult. Therefore, you can have chronic hypoxemia and also have hypocapnia due to tachypnea. Tachypnea is a response from the Peripheral Chemoreceptors detecting chronically low pO2 levels, but this hypoxemic tachypnea is overridden by the hypocapnia that results which stops the tachypnea even before your pO2 levels are increased past 40mm Hg. Remember: the control pO2 exerts on ventilation is very weak, it basically stops once you get past 40 mmHg. At that point in ventilation, we will probably already have hypocapnia, which exerts a negative ventilatory control through the central chemoreceptors in the medulla. Reference the chart in #15. Pathophysiology Cardiogenic Pulmonary Edema Increase in Transmural Pressure, leads to accumulation of excess fluid in the interstitium. Jv=(Pc+πi)-(Pi+πc) Jv=Outward forces-Inward Forces *Increased Transmural pressure results from ↑Outward forces or ↓Inward forces Edema fluid has low protein content Usually whatever flows out of the capillary can be drawn back due to capillary hydro-osmotic gradient. Whatever is left can be cleared by lymphatics. Symptoms V/Q Ratios Pulmonary Tests Mild Dyspnea (due to C fiber activation) Nonproductive Cough Compliance falls Tachypnea and ↑Work of Breathing Breath Sounds: Rales, Crackles, Rhonchi Wheezing may occur Frothy Sputum (from protein)in the case of a productive cough Low V/Q ratios N/A Noncardiogenic Pulmonary Edema Increased Pulmonary Capillary Permeability or Alveolar Epithelial Permeability, leads to accumulation of fluid in the interstitium. Example: ARDS (Acute Respiratory Distress Syndrome) Destruction of Epithelial Lining (Type I Pneumocytes), leading to flooding in the alveoli. This results from: 1.) Inhaled Toxinsepithelial damage 2.) Circulating Toxinsendothelial damage and eventual epithelial damage Fibrosis and Hyperreactivity Surfactant ↓ (↓Compliance) Leads to Alveolar Edema, Alveolar Hemorrhage, Atelectasis Edema fluid has high protein content Damage to the endothelium leads to leakage of protein into the interstitium. However, this doesn’t lead to alveolar flooding because the alveolar epithelium is completely impermeable to protein, leading to a powerful osmotic gradient that keeps fluid in the interstitium. However, in later stages this barrier is breached and we get alveolar flooding. Dyspnea Compliance falls Tachypnea Low V/Q ratios, High V/Q ratios N/A Compliance Inflammation Hypoxemia ↓ No Yes ↓ Yes Yes Hypocapnia Hypercapnia Can be low due to tachypnea No, Normal or Low PaCO2 levels No Yes, due to increasing dead space ventilation Stages of Pulmonary Edema: Stage 1: Eccentric Fluid Accumulation Stage 2: Crescentic Filling of Alveoli And Peribronchovascular Intersitium Distention (When edema is greater than what the lymphatics can remove) Stage 3: Alveolar Flooding Pathophysiology Pulmonary Embolism Obstruction of Perfusion by a moving clot (Same Risk Factors as DVT) ↓Surfactant due to hypoperfusion (which interferes with surfactant production in type II cells) Leads to Alveolar edema, collapse, and atalectasis Symptoms Dyspnea Pleuritic Chest Pain Hemoptysis Tachypnea Increase in Pulmonary Arterial Pressure (due to hypoxemia) V/Q Ratios High V/Q ratios (Classic Example of Alveolar Dead Space) Low V/Q ratios (due to ↓surfactant and ↓compliance) Angiography, there is a “hole” ↓ No Yes Possible Yes, due to increasing alveolar dead space Pulmonary Tests Compliance Inflammation Hypoxemia Hypocapnia Hypercapnia