Even
advertisement

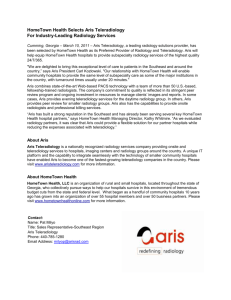
Annie Garrigus 10/10/11 Ecosystem Mini-Project Teleradiology: Evolving Technologies and Business Models With an aging population, an increase in people living with chronic diseases, and rising healthcare spending, the U.S. needs ways to improve the quality and reduce the cost of care. Teleradiology exemplifies one such solution. Though the technology has been around since the 1990s, major improvements in network speed and security have allowed teleradiology to provide greater efficiencies in recent years. This analysis will focus on teleradiology in the U.S. market with specific focus on the business model of Virtual Radiologic Corporation, or vRad. VRad seized the number one position in the U.S. market for teleradiology services when it merged with the market leader, NightHawk Radiology Holdings, Inc. (“NightHawk”), in December 2010. Both vRad and NightHawk were publicly-traded companies with $172 million (as of 8/7/08) and $130 million (as of 10/16/08) market capitalizations, respectively, during 2008. Virtual Radologic was taken private in July 2010 when it was acquired by Providence Equity Partners. Diagnostic Imaging Diagnostic imaging describes non-invasive procedures used to take pictures of internal anatomy and processes using film or digital technologies. These pictures and videos are used to diagnose a wide range of medical conditions on an emergency or non-emergency basis. There are several types, or modalities, of diagnostic imaging including computed tomography (CT), magnetic resonance imaging (MRI), positron emission tomography (PET), radiography (X-rays), ultrasound, and mammography. Diagnostic imaging services are increasing faster than the supply of radiologists. These scans can be a way to rule out the need for more invasive procedures, reducing cost and amount of care. The growing demand for imaging combined with the shortage in radiologists necessitates more efficient radiology services. Teleradiology Teleradiology is the practice of sending digital medical images from the imaging site to a remote location for study by a radiologist. Traditional radiology services require a radiologist to live near a hospital or medical practice where he is employed or affiliated and travel there to interpret images. Teleradiology allows 1 the radiologist to receive images at an off-site location – a home office or centralized reading center – in an encrypted format via a fast and reliable connection. In the 1990s, teleradiology was mainly used in emergency situations to send scans to radiologists at home. Today, teleradiology companies – essentially virtual radiology practices – have emerged. These practices consist of radiologists located off site across the country or world who are licensed and credentialed across multiple hospitals and states. They submit reports to the site of care often faster than on-site radiologists could do so given their administrative duties and other on-site distractions. According to a 2004 Radlinx Group survey, 87% of radiology practices that responded used teleradiology. In other words, they were able to receive and read diagnostic images electronically. They did not necessarily contract with an outside teleradiology company. Even after the merger of the number one and two players, the teleradiology market remains fragmented with many small, private companies. Companies are differentiated by their ability to recruit and retain radiologists as well as obtain licenses and credentials for employed physicians in many states. The market opportunity remains attractive, as a 2008 Frost and Sullivan report estimates continued growth of the U.S. Marketing for Teleradiology Services at 15% annually. Radiology Service Providers There are two primary sites for radiology services – hospitals and radiology clinics. Hospital radiology services are usually provided by a radiology practice, a group of affiliated radiologists, that contracts with the hospital and determines the staffing schedule. Depending on the size, a radiology practice may provide coverage for one or more hospitals. Radiology practices may also operate independent clinics that receive referrals from other physicians. To manage night shifts when fewer radiologists are on site and periods of high demand, some radiology practices enter into contracts with teleradiology companies. The imaging site sends digital images to the teleradiology company which assigns each study (set of images) to one of its radiologists (often referred to as a telerad). The telerad interprets the images and sends a report back to the on-site radiology practice. These steps require the use of both general and proprietary technologies. Technology that Enables Teleradiology In order to send images between imaging sites or from an imaging site to teleradiology company for reading, facilities must be equipped with picture archiving and communication systems (PACS), computers or networks that store, retrieve, distribute, and present images. PACS are used in lieu of film and fullcapability PACS can handle images from all modalities. Customers send PACS data to outsourced providers via a reliable and secure Virtual Private Network (VPN). 2 DICOM (digital imaging in communication) is a set of industry standards that allows for the transfer of medical images and information between computer networks and diagnostic imaging equipment made my different manufacturers. Hospital and radiology practices can choose between many different PACS that are compatible with DICOM to be able to take advantage of teleradiology services. The teleradiology provider may assist the radiology site in determining the best PACS for its needs. When teleradiology companies receive a set of images for a patient, their workflow management systems immediately assign the study to a telerad based on a set of criteria. The criteria depend on the workflow system and may include backlog, licenses, credentials, and subspecialty areas. The Virtual Radiologic Business Model Before merging with NightHawk in December 2010, Virtual Radiologic maintained a network of radiologists located almost entirely in the U.S. The company enters into two-year contracts with radiologists that automatically renew unless broken by either party. Almost all radiologists work out of home offices, reading images primarily between the hours of 8pm and 10am. Radiologists tend to work 7 nights in a row then take 7 nights off. They perform both preliminary and final reads, though preliminary represent the majority. A preliminary read is an initial diagnosis made shortly after the image is generated. A final read is a more thorough analysis, taking into account the patient’s history and providing a more detailed reading of the image with measurements and other specifics. Only final reads are reimbursed by Medicare and commercial insurers. When interpreting a set of images, a telerad may want to speak with the referring physician to get additional patient information and provide a better report. VRad has an operations center that connects telerads to referring physicians, minimizing the time it would take a telerad to track down a referring physician on his own. The NightHawk model differs based on the geography of the radiologists and the location of work. NightHawk operates two centralized reading centers in Zurich, Switzerland and Sydney, Australia. Most radiologists have relocated from the U.S. and they have U.S. licenses and credentials and U.S. hospitals. NightHawk radiologists can work local daylight hours while reading scans for U.S. hospitals, clinics, and imaging centers during their overnight hours. NightHawk only performs preliminary reads, as insurers require that final reads be performed by U.S.-based physicians. Other companies locate radiologists overseas in lower-cost labor markets such as India. However, physicians must be licensed in the state and credentialed by the hospital from which the scan was sent to interpret the scan of a U.S. patient. 3 Doctors who have the same training, licenses, and credentials as U.S.-based radiologists will demand similar compensation, so there is little benefit to locating telerads in these markets. For both vRad and NightHawk, most scans are received from clients’ emergency rooms. Greater than 75% of the orders received are CT scans. Telerads are able to provide preliminary readings in 15-20 minutes vs. an average of 30 minutes for on-site readings. They typically provide final reads within 24 hours vs. 72 hours on-site. More than 75% of vRad radiologists are subspecialty trained. The Virtual Radiology business model relies on several proprietary applications. In early 2010, vRad’s request for a patent covering its workflow, order forecasting, and radiologist scheduling applications was approved. Its workflow technology called “Multiple Resource Planning System” receives images (in groups called orders) over the Internet and applies rules to allocate orders to radiologists based on subspecialty training, licensing, credentialing, workload, hospital preferences and other factors. The vRad PACS is a cloud solution, hosted and managed on the Internet. VRad also offers cloud storage for digital images through its vRad Vault product. The company now licenses these applications to radiology practices. The technology especially helps practices that cover multiple facilities (hospitals or clinics), allowing them to “load balance,” or even out the orders assigned to radiologists at different sites. Teleradiology Value Vision The primary value of teleradiology is the ability to scale limited radiologist resources to accommodate the increasing volume of diagnostic images. Teleradiology provides additional coverage during periods of high demand and overnight when hospitals are thinly staffed. Over 50% of emergency diagnostic imaging takes place at night, when fewer radiologists are on duty. Without teleradiology, on-site radiologists would have to work longer and less desirable hours. Otherwise, turnaround time for reads would deteriorate, hurting patient outcomes in emergency situations. On average, telerads provide quicker turnarounds of initial and final reads than their on-site counterparts. Telerads are able to be more productive due to advanced workflow management applications that provide them with a steady supply of orders to interpret, spreading the work as evenly as possible across telerads on duty. Telerads do not have any administrative duties or distractions that consume on-site radiologists’ time. Teleradiology provides another significant benefit to radiology practices that lack a range of specialties, namely smaller and rural hospitals and clinics. It is difficult for 4 one practice to attract a full complement of subspecialists, but teleradiology provides such access. Workflow management systems are able to efficiently allocate cases to subspecialists when appropriate. The software teleradiology companies sell to help radiology practices manage information and scans also provide significant value. VRad’s solution, vRad Enterprise Connect, provides the platform to manage, read and store studies. It compiles information from different locations and radiology technologies onto one platform for workflow management. VRad also offers an Internet-based Radiology Information System (RIS), including fully integrated voice dictation. These products make radiologists more productive, improving patient care and lowering costs. Aligning the Actors in the Teleradiology Ecosystem The teleradiology ecosystem consists of teleradiology companies, teleradiologists (telerads), radiology practices, hospitals, referring physicians, insurers (public and private), and patients. The role, incentives, and benefits for each are outlined below. Radiology practices are the key actor that must see the benefit in teleradiology, as the practices contract with the teleradiology companies. However, as vRad shifts its business model over time, payors and hospital systems will be the most important actors, as they stand to gain from efforts to control costs. Teleradiology companies are taking advantage of the growing need for productive radiology interpretation services, as the growth in diagnostic imaging is outpacing the growth in radiologists. Currently, these companies have a fee-forservice model. They receive most of their revenue directly from radiology practices, as the majority of reads are preliminary and not eligible for reimbursement by insurers (payors). As vRad and other teleradiology companies with U.S.-based doctors perform more final reads, they will benefit from higher margins but also incur more direct exposure to payors. As reimbursement rates decline for radiology services, so do the fees collected by teleradiology companies. Technology licensing fees represent a small percentage of total revenue (less than 10%), but they are growing and help to offset compression in service fees. Teleradiologists are attracted to the higher potential compensation and more flexible schedule associated with teleradiology. As telerads are more productive than on-site radiologists, receiving and reading more images per hour, they generally have higher annual incomes. One Bank of America analyst report estimates that the average NightHawk telerad collects $600,000 per year vs. $300,000 to $400,000 for the average on-site radiologist. The typical vRad schedule of 7 nights on, 7 nights off provides flexibility to take vacations and pursue other interests. Doctors typically enter into contracts with vRad for 1,600 to 5 2,200 hours per year which translates to a reasonable 33-46 hours per week assuming 4 weeks of vacation (48 working weeks a year). VRad radiologists have the flexibility to work from home and live anywhere in the U.S. They also have the ability to see a higher volume of images in their subspecialties given the superior workflow management. Radiology practices, both hospital-based and independent, are able to provide the level of coverage required to maintain service contracts (with hospitals or physician groups) by contracting with teleradiology companies. They are also able to better attract and retain radiologists, which are in high demand, by not requiring them to work overnight shifts or weekends. Practices also benefit from licensing a teleradiology company’s proprietary software because it allows them to better balance workload among sites and radiologists. Licensing software also saves practices the capital expense required to develop their own solution. Hospitals generally prefer to have doctors on site, but teleradiology is the next best option, allowing access to productive resources during a time when 50% of emergency scans take place. Telerads are likely to be more awake than those working overnight shifts, resulting in more accurate reads. Ideally, hospitals should see that teleradiology results in improved patient care - faster reads by nonfatigued radiologists with greater access to subspecialists. In reality, though, hospitals tend to view teleradiology as a necessary evil – the necessary alternative to having doctors on site Referring physicians, the doctors treating the patients who receive diagnostic imaging procedures, have little say in contracting with teleradiology companies unless such contracting yields inferior results. They may prefer the faster turnaround time teleradiology provides, allowing them to diagnose and treat patients more quickly, improving outcomes. Teleradiology also allows them to get copies of imaging reports on their iPhones or computers to use real-time. These benefits should outweigh the drawbacks of being able to have a face-to-face discussion with a colleague in the radiology department. Payors (Medicare, Medicaid, and private insurers) are essentially indifferent between on-site radiology and teleradiology given the current fee-for-service model, as cost is similar. Ideally, payors would recognize teleradiology’s ability to provide higher quality care. If teleradiology companies like vRad migrate to a fixed rate model, payors stand to benefit. Patients benefit from teleradiology’s ability to provide quicker reads, especially in emergency situations. Faster turnaround times facilitate faster diagnoses. Patients 6 benefit from higher quality reads by non-fatigued doctors with a range of subspecialties. As patients rarely interact with radiologists, they do not miss the face-to-face communication. Evolution of vRad’s Business Model In response to fee compression faced by radiologist practices that gets passed onto teleradiology companies, vRad aims to transform its business model from fee-forservice to fixed rate on a per member basis. VRad seeks to contract directly with independent physician practices, hospital networks, and payors. VRad would quote a fixed rate per member (patient) to manage all radiology costs. This model requires vRad to have on-site radiology groups in addition to telerads. VRad would get more volume from exclusive contracts, and customers would benefit from predictable (fixed) costs, better care, and more satisfied members. Managing a patient for a fixed cost rather than receiving a fee for each imaging event would incentivize vRad to maximize radiologist productivity and accuracy, containing costs and lessening the likelihood that a patient will receive additional imaging. The key challenge to this transition is the need to ultimately displace vRad’s current customers – radiology practices – which currently contract with hospitals and payors. VRad plans to make this transition gradual, starting with large physician groups, which do not overlap with radiology practices’ current market. VRad will need to convince current and potential customers that the new model offers more benefits than the existing one. 7 Teleradiology Ecosystem Teleradiologists (telerads) Teleradiologist Companies (e.g. vRad) Limited interaction with payors to get reimbursed for final reads contract Send patients for radiology services Radiology Practices Reimbursement for “professional” part of imaging bill Referring Physicians Return reports used for diagnosis and treatment contract Hospitals Reimbursement for “hospitall” part of imaging bill Payors 8