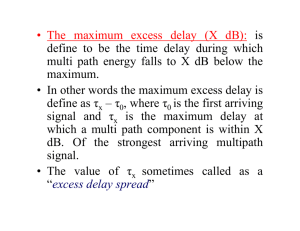
TTE Additional Imaging Views for Pathology (Adult)
advertisement
")
TTE Additional Imaging Views for Pathology (Adult) Standard E5 Preamble Besides the standard imaging views completed for a normal TTE study, additional views are required to help determine a diagnosis when pathology is present. Describe the laboratory protocols for abnormal pathology. Aortic Stenosis PLAX: Standard AV view with m mode to display timing of valve opening, and closing and thickness of cusps. Use of the zoom feature on the valve for careful AV root visualization and measure. 2D diameter measurements of the Sinus of Valsalva, sinotubular junction and ascending aorta. PSAX: AV 2D imaging using the zoom feature. Adjustment of controls to enhance endocardial definition. Adjust angle of view to ensure all 3 cusps are clearly viewed. Planimetry of the valve. APICAL 5ch: Zoom-in feature on 2D image of AV and LVOT. Assess color by Doppler, any eccentricity of flow. PW of the LVOT at the level of the cusps. CW Doppler through the most turbulent flow of the AV color jet, for PPG and MPG. Vena contract to assess AR severity. ERO. Pedoff (non-imaging transducer) flow velocity. ALAX (Apical 3ch): 2D of AV function. Color flow Doppler. CW through AV. Subcostal Alternate view: AV SAX showing the aorta, turn color on and place CW cursor in the most turbulent flow, for PPG/MPG. Suprasternal: Arch view concentrating on the ascending aorta: turn on the color and complete a CW Doppler and pedoff measurement for PPG and MPG. Right Sternal Border: Turn patient on their right side and image the ascending aorta from the RPLAX view, turn the color on and find the turbulent area of the color flow using CW and/or pedoff probe— measure for the maxim PPG and MPG. Pericardial Effusion PLAX: Set the depth setting to identify pericardial or pleural effusions. Measure the diameter of the fluid during diastole from different points. Assess for pericardial fat or thrombus. PSAX - LV/RV: Set depth setting to view around the LV and the RV. Measure the diameter of the fluid from different points, during diastole. PSAX - AV/PV: Doppler the pulmonary outflow with pulsed wave and a slow sweep speed to view variation with respiration in the Doppler spectral waves. Turn respirometer on—leave on for duration. Assess for fluid and measure. Apical 4 Chamber View: Set depth setting to ensure all 4 chambers are completely viewed. Measure fluid from different points around the heart during diastole. Look for effects on the RV and RA. Place m mode cursor through the RA and time collapse of the RA free wall between R-R. Doppler MV inflow with pulsed wave and a slow sweep speed to watch for respiratory variation. Doppler TV concentrating on the E wave size, slow sweep speed and respiratory variation. Apical 5 Chamber View: Doppler the AV LVOT with PW on a slow sweep speed and assess for respiratory variation. Subcostal view: Depth setting to see all around the heart. Complete measurements at various points around the heart during diastole. If RV collapses, place m mode through the RV free wall, through the IVS and through the LV to display the RV free wall movement to time the severity of the collapse. SAX: Measure IVC plethora and complete sniff test to assess collapsibility. Pulse on the hepatic flow. Document: Location of fluid: located, circular. Diameter range from the views: circular pericardial effusion measuring 1.5 to 2 cm with the highest measurement by RA. Signs of tamponade: RV collapse throughout the R-R cycle. Note: Most pathologies will require additional views and measurements hence the lab should have criteria in place to demonstrate the expected information to be obtained.