Population Genetics 2nd Assignment REV
advertisement

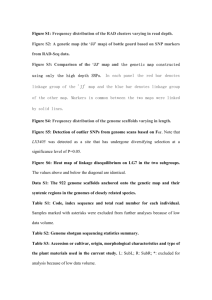
MAPPING BY ADMIXTURE LINKAGE DISEQUILIBRIUM: ADVANCES, LIMITATIONS AND GUIDELINES The main principles in this paper that have also been addressed in lectures are linkage disequilibrium and admixture. Firstly, linkage disequilibrium is the non-random association of alleles on different loci, which have ancestral origins on the same chromosome. As a result, these alleles are not independent of each other. Secondly, admixture is the process of interbreeding between two previously genetically divergent populations, which gives rise to a new population. The offspring can then interbreed with the parental populations to provide more genetic variation. These two processes can be viewed together as admixture linkage disequilibrium. The new genetic variants that result from admixture have massive gene flow that can be studied closely. There is linkage disequilibrium between all loci with high allele-frequency differences between the parental populations. In this paper, mapping by admixture linkage disequilibrium (MALD) is being tried as a new approach for studying and mapping genetic variants associated with human disease. In particular, it studies the long-range haplotypes that are formed as a result of recent admixture in AfricanAmerican and Latino populations. This paper does not address a hypothesis/alternative hypothesis explicitly, however, alternative methods to MALD are addressed, including linkage mapping and genetic association mapping. Linkage mapping can only be used for rare, monogenic, Mendelian family-studies and although genetic association mapping can be used for complex diseases, the process requires many more markers and can often be expensive. This paper explains that MALD would be less expensive as it includes only around 2000 markers, but will also have greater accuracy when studying the effects of multiple genes on a complex disease. What makes MALD different to other genetic associations studies is that only the genomes of individuals who have mixed ancestry and who suffer from diseases of interest are eligible to take part. The people who fit these inclusion criteria are then progressed further in the study. The sample sizes required to make a statistically sound estimate of disease-associated alleles varies depending on the initial parental ancestries and the disease in question. As MALD is a new approach, there are no definitive results, only estimates at the sample sizes. Instead this paper addresses the theory behind it and the possible future implications. Genotype data were collected from human individuals who were of mixed ancestry, and were also affected by a disease of interest. These, and control cases, were then screened against a set of polymorphic markers. These markers allow you to determine the ancestry of individual genes in the whole genome. Additionally, chromosomal regions that have higher than average disease-gene incidences are identified. From all of this, the disease-causing alleles can be determined by studying the high incidence of nearby SNPs.