ELECTIVE ROUTINE URGENT EMERGENCY P
advertisement

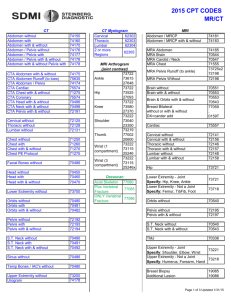
Request for Out Patient Imaging Patient Information Name (LAST, FIRST, MIDDLE INITIAL) DOB DATE SEX General instructions - All orders for clinical exams or tests must include a statement of medical necessity by ICD –9/10 code or M F diagnosis. Test not covered by that code may be charged to the patient. Please check the box next to the appropriate exam and code and write ICD 9/10 code is space provided at bottom of the form. Please read and check the contrast statement located below. Pt. SSN Referring Physicians Signature ORDERS VALID FOR 30 DAYS FROM DATE OF SIGNING Please use ALL Pre-Cert Codes for insurance pre-certifications ALLOW USE OF CONTRAST AT THE DISCRETION OF THE RADIOLOGIST CAT SCAN EXAM CONTRAST USED AT THE DISCRETION OF THE RADIOLOGIST 70450/70460/70470 70450/70460/70470 70486/70487/70488 70480/70481/70482 70486/70487/70488 CONTRAST USED AT THE DISCRETION OF THE RADIOLOGIST EXAM PRE-CERT CODES HEAD BRAIN FACE ORBIT IAC MRI _ _ EXTREMITY SPECIFY ____________________ UPPER 73200/73201/73202 LOWER 73700/73701/73702 NECK 70490/70491/70492 CHEST 71250/71260/71270 ABD / PELVIS 74176,74177,74178 STONE PROT 74176 PELVIS (ORTHO)72192/72193/72194 SPINE CERVICAL 72125/72126/72127 THORACIC 72128/72129/72130 LUMBAR 72131/72132/72133 CTA STUDY OF; PRE-CERT CODES BRAIN IAC ORBIT PITUITARY SPINE CERVICAL THORACIC LUMBAR NECK PELVIS EXT. UPPER-SPECIFY_ 70551/70552/70553 70553 70540/70542/70543 70553 72141/72142/72156 72146/72147/72148 72148/72149/72158 70543 72195/72196/72197 73218/73219/73220 UPPER-JOINT SPECIFY 73221/73222/73223 ______________ EXT. LOWER-SPECIFY 73718/73719/73720 LOWER JOINT SPECIFY 73721/73722/73723 BREAST BREAST LEFT RIGHT BILATERAL 77058 77059 YES NO ULTRASOUND NUCLEAR MED EXAM EXAM PRE-CERT CODES RUQ 76705 ABDOMEN 76700 RENAL 76775 PELVIS 76856 OB-COMPLETE >14WKS 76805 OB-LIMITTED 76815 OB-F/U 76816 BIO – PROFILE 76818 PELVIC/TRANSVAGINAL 76830-76857 CAROTID BILAT 93880 VENOUS Doppler: Bilat 93970/Uni 93971 Upper Lower ART. Doppler:Upper Bilat 93930 Uni 93931 Lower Bilat 93925 Uni 92926 BREAST RT 76645 LT 76645 SCROTUM 76870 w/Doppler 93975 PYLORUS 76705 BIOPSY OF MRA--SPECIFY BIOPSY OF: OTHER OTHER CALL 522-5015 TO SCHEDULE VASCULAR / ECHO EXAM OTHER PRE-CERT CODES CALL 522-5015 TO SCHEDULE ANGIO INTERVENTIONAL PRE-CERT CODES CARDIAC STRESS BONE SCAN 3 PHASE BONE SCAN SPECT LUNG SCAN VENT / PERF HIDA I 123 THYROID UPTAKE AND SCAN I 131 THYROID THERAPY I 131 WHOLE BODY SCAN GASTRIC EMPTYING STUDY PARATHYROID SCAN SENTINEL NODE INJECTION WHITE BLOOD CELL GALLIUM STUDY MUGA STUDY G.I.BLEED STUDY LIVER / SPLEEN STUDY HEMANGIOMA STUDY MECKEL’S STUDY RENAL STUDY 79005 78306 78264 78070 38792 78806 78804 78472 78278 78215/78216 78205/78206 78290 78700/78701 OTHER CALL 522-5015 TO SCHEDULE XRAY CALL 522-5015 TO SCHEDULE ICD 9 DIAGNOSIS CALL 522-5039 TO SCHEDULE ALL ANGIO EXAMS WRITE REQUESTED EXAM IN BLOCK BELOW SEGMENTAL 93923 PPG 93965 ABI 93922 ECHO 93306 TEE 93312 CALL 522-5015 TO SCHEDULE 78452/78453 78306/78320 78306/78320 78580 78596 78223 78006 CALL 522-5015 TO SCHEDULE CALL 522-5015 TO SCHEDULE