anterior neck/nasopharynx
advertisement

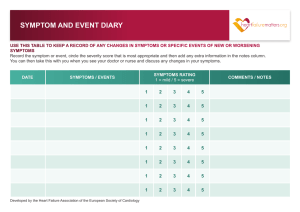
ANTERIOR NECK/NASOPHARYNX Last Name: _____________________________ First Name: __________________ Date: ______ 1. Have you had a CT scan of the area of interest? _______________________________________ If yes, when __________________________ What did it show? ________________________ 2. What does your doctor think may be causing your problem? _____________________________ ____________________________________________________________________________ ____________________________________________________________________________ 3. Describe your symptom (pain, mass, weight change, etc.)________________________________ ____________________________________________________________________________ 4. Does anything make the symptoms worse? _________________________________________ ______________________________________________________________________________ 5. Does anything make them better? _________________________________________________ _____________________________________________________________________________ 6. Have you had a biopsy or surgery? ______________ When? ____________________________ What was done? ________________________________________________________________ Results? _______________________________________________________________________ 7. Are you taking any medicines? □ Yes □ No If yes, what kind: _______________________________________________________________ ____________________________________________________________________________ 8. Do you have any other medical conditions? □ Yes □ No If yes, what? ___________________________________________________________________ 9. Describe your general health: _____________________________________________________ PLEASE COMPLETE BOTH SIDES