1. Determination of vancomycin concentration
advertisement

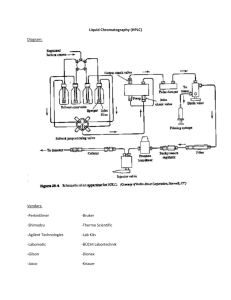
Supplemental Digital Content A Larger Dose of Vancomycin Is Required in Adult Neurosurgical Intensive Care Unit Patients Due to Augmented Clearance The HPLC assay was validated regarding its linearity, limit of quantitation, accuracy and imprecision (intra- and inter-day) in this supplementary data. Materials and Methods 1. Determination of vancomycin concentration 1.1 Patient sample collection After signing the informed consent, patients of NSICU ward fitting the inclusion criteria were collected into our study. Vancomycin TDM is ordered after achieving steady state (defined as after the fourth dose). Twenty-four hour urine and CSF collection began on TDM day, an aliquot of 40 mL of patient sample was collected in centrifuge tubes on the morning after TDM day. Samples were centrifuged at room temperature,1699 g for 15 min, supernatant was stored in -80℃condition until analysis. 1.2 Standard solution preparation Stock solutions of vancomycin were prepared at 5.0 mg/mL in double-distilled water (ddH2O). Working solutions were prepared by serial dilution of stock solution to concentration levels of 3.0 – 4000 mg/L. All solutions were stored at -20℃ and brought to room temperature before use. Calibrators were prepared by spiking working solutions into blank human urine or CSF. For the preparation of urine calibration standard, 30 μL of working solution (concentrations 100, 200, 300, 600, 1000, 2000, 3000, 4000 mg/L) was spiked into 270 μL blank urine to make final concentrations of 10, 20, 30, 60, 100, 200, 300, 400 mg/L vancomycin in urine. For the preparation of CSF calibration standard, 30 μL of working solution (concentrations 3, 10, 20, 30, 60, 100, 200, 300 mg/L) was spiked into 270 μL blank CSF to make final concentrations of 0.3, 1, 2, 3, 6, 10, 20, 30 mg/L vancomycin in CSF. Quality control solutions for recovery test were prepared by the same method to obtain the following concentrations: 30, 100 mg/L in urine and 3, 10 mg/L in CSF. Quality control solutions for accuracy and precision validation were prepared by the same method to obtain low, medium and high concentrations; 20, 60, 300 mg/L in urine and 1, 6, 30 mg/L in CSF. 1.3 Sample preparation Urine and CSF samples were removed from -80℃and brought to room temperature. Sample preparation was done by two steps: organic solvent precipitation of proteins (de-protein), followed by liquid-liquid extraction. For the sample preparation of urine, an aliquot of 300 μL urine was transferred to an 1.5 mL eppendorf and thoroughly mixed with 300 μL of de-protein reagent, acetonitrile/isopropanol (50/50, v/v). The solution was centrifuged at 4℃, 4487 g for 10 min. 500 μL of supernatant was collected and air dried in chemical hood at room temperature. Afterwards, the sample was reconstituted by 250 μL ddH2O, followed by extraction with 1.0 mL of chloroform. Finally, 150 μL of upper aqueous phase was ® collected, and filtered by Minisart RC-4 0.2 μm membrane. Injection volume of 20 μL was injected into HPLC system. For the sample preparation of CSF, an aliquot of 300 μL CSF was transferred to an 1.5 mL eppendorf and thoroughly mixed with 300 μL of de-protein reagent, acetonitrile/isopropanol (50/50, v/v). The solution was centrifuged at 4℃, 4487 g for 10 min. 500 μL of supernatant was collected and air dried in chemical hood at room temperature. Afterwards, the sample was reconstituted by 250 μL ddH2O, followed by extraction with 1.0 mL of chloroform. 150 μL of upper aqueous phase was collected, and centrifuged again at room temperature, 4487 g for 10 min. Finally, sample was filtered by Minisart® RC-4 0.2 μm membrane. Injection volume of 20 μL was injected into HPLC system. 1.4 High Performance Liquid Chromatography (HPLC) conditions The reverse phase HPLC system consisted of a Hitachi Model L-2130 pump, Model L-2200 autosampler, Model L-2300 column oven, and Model L-2420 UV-Vis detector. Systems manager and data analysis relied on Hitachi Model D-2000 Elite Chromatography Data Station Software. A reverse phase Agilent Zobrax SB-C18 analytical column (4.6 mm ID x 250 mm, 5 μm) was used, equipped with a pre-column Phenomenex® Security Guard C18 KJ0-4282 (4 x 3.0 mm ID). Mobile phase consisted of 100 % acetonitrile (solvent A) and 30 mmol/L potassium dihydrogen phosphate (KH2PO4) buffer, adjusted to pH 4.0 by H3PO4/KOH (solvent B). Column oven temperature was set at 30℃, UV detection wavelength was set at 220 nm. The chromatographic separation conditions for vancomycin in urine are as follows: linear gradient 7 % to 17 % solvent A in 10 minutes; 17 % to 50 % solvent A from 10 to 11 minute; maintain 50 % solvent A from 11 to 16 minute; 50 % to 7 % solvent A from 16 to 18 minute; maintain 7 % solvent A until 23 minute. Flow rate was set at 1.0 mL/min, injection volume was 20 μL per sample. The chromatographic separation conditions for vancomycin in CSF are as follows: linear gradient 7 % to 14 % solvent A in 11 minutes; 14 % to 50 % solvent A from 11 to 13 minute; maintain 50 % solvent A from 13 to 18 minute; 50 % to 7 % solvent A from 18 to 20 minute; maintain 7 % solvent A until 24 minute. Flow rate was set at 1.0 mL/min, injection volume was 20 μL per sample. 1.5 Concentration determination in patient sample Calibration curves were built for the concentration determination of vancomycin in urine and CSF. Calibrator solutions were prepared as described in 1.2. Triplicate (n = 3) repeat was performed for each concentration within run and between run on 3 different days. Concentration versus HPLC peak response area was plotted, and linear regression was performed to build calibration curve. For concentration determination, patient samples were first prepared as described in 1.3 and injected into HPLC system to detect the HPLC peak response area. Each sample injection was performed in triplicate (n = 3) repeats. The response area was applied to the calibration curve to determine the concentration. Mean ± standard deviation concentration was calculated. 1.6 Validation of HPLC assay The assay was validated regarding its linearity, limit of quantitation, recovery, accuracy and imprecision (within run and between run). Linearity was determined by the regression coefficient value. Limit of detection was defined as 10 times signal-to-noise level. Quality control solutions for recovery validation were prepared as described in 1.2. Triplicate (n = 3) repeat was performed for each concentration. In the recovery tests, HPLC peak response from quality control solutions was compared with peak response of aqueous solution spiked with equal vancomycin concentrations. Quality control solutions for accuracy and precision validation were prepared as described in 1.2. Triplicate (n = 3) repeat was performed for each concentration within run and between run on 3 different days. For accuracy validation, the concentrations were recalculated from the corresponding calibration curve and compared with the theoretical concentrations. For precision validation, we looked at the coefficient of variation (CV %) of recalculated concentrations. In addition, the correlation data between the FPIA and the HPLC method was performed by the comparison of the vancomycin concentration. Results 1. HPLC-UV assay development 1.1 Assay condition determination and building calibration curve The assay condition yielded an optimal separation of vancomycin, the retention time was about 8.8 minutes in urine, and 9.2 minutes in CSF. Because different concentration ranges of vancomycin were expected in urine and CSF samples, the linear range of the calibration curve was different. The linearity range for vancomycin detection in urine was 10 – 400 mg/L; the calibration curve showed optimal linearity with a R2 = 0.9996. The linearity range for vancomycin detection in CSF was 0.3 – 30 mg/L; the calibration curve also showed optimal linearity with R2 = 0.9971. Other calibration curve parameters are shown in Table 1. 1.2 Assay validation The HPLC assay developed in this study was validated regarding its linearity, limit of quantitation, recovery, accuracy and precision (within run and between run). The validation parameters are shown in Tables 1 – 3. The limit of quantitation reached 10 mg/L in urine, and 0.3 mg/L in CSF. The recovery tests were performed on quality control samples at two concentration levels; recovery tests for urine and CSF were inside the 90 – 110 % range. The within run and between run accuracy and imprecision were determined by analyzing quality control samples at three concentration levels; the within run and between run accuracy and precision were also acceptable. We compared vancomycin determinations by HPLC and FPIA in a small numbers of plasma samples. The concentration differences between these two methods in most samples were below 15%. Pearson correlation reveals the correlation coefficients between these two methods for vancomycin was 0.94 (Figure 1). Based on the results, the concentrations obtained by the two methods were considered comparable. Table 1. Linearity and quantitation limit of HPLC assay Linearity range Vancomycin Calibration curve parameter LOQ (mg/L) Slope Intercept R2 (mg/L) 10 - 400 41043 121868 0.9996 10.0 0.3 - 30 42117 20930 0.9971 0.3 in urine Vancomycin in CSF Abberviations: LOQ, lower limit of quantitation; CSF, cerebrospinal fluid Triplicate (n = 3) repeats were performed for each concentration within run and between run, on 3 different days. LOQ is defined as the concentrations which yield a measure peak with signal-to-noise ratio (S/N) of 10. Table 2. Recovery validation parameters of HPLC assay Quality control Recovery concentration (mg/L) (%) Vancomycin in urine 100 102 30 110 Vancomycin in CSF 10 108 3 110 Abberviations: CSF, cerebrospinal fluid Triplicate (n = 3) repeats were performed for each concentration within run and between run on 2 different days. The data was pooled to calculated average recovery. Table 3. Accuracy and precision validation parameters of HPLC assay Quality control concentration (mg/L) Within run Mean Between run Accuracy CV Mean determined determined concentration concentration Accuracy CV (mg/L) (%) (%) (mg/L) (%) (%) 300 308.7 103 1.30 311.9 104 0.90 60 62.6 104 2.42 61.3 102 2.52 20 21.4 107 0.66 21.3 106 1.97 30 32.0 107 0.61 32.0 107 0.19 6 6.1 102 2.97 6.2 103 0.34 1 0.98 98 0.80 0.96 96 0.11 Vancomycin in urine Vancomycin in CSF Abbreviations: CV, coefficient of variance; CSF, cerebrospinal fluid Triplicate (n = 3) repeats were performed for each concentration within run and between run, on 3 different days. Figure 1. The correlation of vancomycin concentrations measured by the FPIA and HPLC.