2002 hospital core measure selection form
advertisement

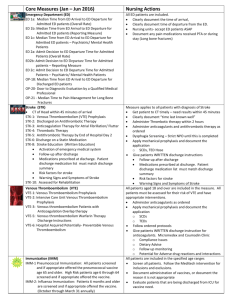
The Joint Commission 2015 FLEXIBLE ORYX REPORTING OPTIONS and CORE MEASURE SET SELECTION FORM HCO ID# Fax Completed Forms to (630) 792-4992 HCO NAME ADDRESS CITY, STATE, ZIP 2015 ORYX REPORTING OPTIONS Effective with January 1, 2015 discharges accredited hospitals have the flexibility of meeting their ORYX measure reporting requirements through one of three options. Detailed information regarding each of the available reporting options can be found in the “2015 Flexible ORYX Performance Measure Reporting Options” document posted under the “Measurement” section of The Joint Commission’s website at http://www.jointcommission.org/performance_measurement.aspx. Please carefully review the options document. Once you have reviewed the 2015 options: Select the one best option for your hospital by checking the appropriate box below. Complete your minimum 6 core measure set selections for 2015 by completing the relevant page(s) that follow o NOTE: Critical Access Hospitals are only required to select a minimum of 4 sets of measures Fax your completed form to 630-792-4992 or e-mail the form to fzibrat@jointcommission.org Provide your listed core measure vendor with a copy of this form. 2015 FLEXIBLE ORYX REPORTING OPTIONS (Select ONE Option) □ Option 1 – vendor submission of quarterly data on a minimum of six sets of chart-abstracted measures. Complete measure set selections using the CHART-ABSTRACTED MEASURE SET SELECTION FORM □ Option 2 – vendor submission of quarterly data on a minimum of six sets of electronic clinical quality measures (eCQMs). Complete measure set selections using the eCQM MEASURE SET SELECTION FORM □ Option 3 – vendor submission of quarterly data on a minimum of six sets of measures using a combination of chartabstracted measure sets and electronic clinical quality measures (eCQM) measure sets. Complete measure set selections using the CHART-ABSTRACTED MEASURE SET SELECTION FORM and eCQM MEASURE SET SELECTION FORM as appropriate. Hospitals wishing to select this option and that may be interested in reporting on the same set(s) of chart-abstracted and eCQM measure sets/measuress should contact Frank Zibrat at 630-792-5992 or via e-mail at fzibrat@jointcommission.org NOTE: Hospitals must continue to meet their ORYX reporting requirements through the selected option for a minimum of calendar year 2015. (Cont’d. on next page) Page 1 of 4 The Joint Commission 2015 CHART-ABSTRACTED CORE MEASURE SET SELECTION FORM HCO ID# Fax Completed Forms to (630) 792-4992 HCO NAME ADDRESS CITY, STATE, ZIP VENDOR SELECTED VENDOR NAME VENDOR ID# DATA COLLECTION START DATE (If changing vendor for 2015) ________________________________________________ ______________ ______________ Data MUST be reported on EACH APPLICABLE MEASURE in the measure set. Data collection must begin on the first day of a calendar quarter. DATA COLLECTION START DATE (If changing measure sets for 2015) □ AMI (AMI-7a) ________________ □ Children’s Asthma Care (CAC) ________________ □ Emergency Department (ED) ________________ □ Hospital Based Inpatient Psychiatric Services (HBIPS) ________________ (AMI-7a) (Unavailable if you do not provide/rarely provide fibrinolytic therapy) (CAC-3) (ED-1a, ED-1b, ED-1c, ED-2a, ED-2b, ED-2c) (HBIPS-1, HBIPS-2, HBIPS-3, HBIPS-4, HBIPS-5, HBIPS-6, HBIPS-7) Data collection required by free-standing Psychiatric Hospitals. Please indicate all patient age groups your organization treats by filling in the appropriate circles. Data must be collected and submitted for all measures and include all relevant patient age groups. o o o o Children (1-12 years) Adolescent (13-17 years) Adult (18-64 years) Geriatric (> 65 years) □ Hospital Outpatient (HOP) ________________ □ Immunization (IMM) ________________ □ (OP-1, OP-2, OP-3, OP-4, OP-5, OP-6, OP-7, OP-18, OP-20, OP-21, OP-23) (IMM-2) Perinatal Care (PC) (Required if the hospital has at least 1,100 live births per year) ________________ (PC-01, PC-02, PC-03, PC-04, PC-05/5a) □ Stroke (STK) ________________ □ Substance Use (SUB) ________________ □ Surgical Care Improvement Project (SCIP) ________________ □ Tobacco Treatment (TOB) □ (STK-1, STK-2, STK-3, STK-4, STK-5, STK-6, STK-8, STK-10) (SUB-1, SUB-2, SUB-3) (SCIP-INF-4) (Unavailable if you do not perform CABG or Other Cardiac Surgery procedures) Venous Thromboembolism (VTE) ________________ (TOB-1, TOB-2, TOB-3) ________________ (VTE-1, VTE-2, VTE-3, VTE-5, VTE-6) (Cont’d. on next page) Page 2 of 4 The Joint Commission 2015 eCQM (Electronic Clinical Quality Measures) CORE MEASURE SET SELECTION FORM HCO ID# HCO NAME ADDRESS CITY, STATE, ZIP Fax Completed Forms to (630) 792-4992 VENDOR SELECTED VENDOR NAME VENDOR ID# DATA COLLECTION START DATE (If changing vendor for 2015) ________________________________________________ ______________ ______________ Data MUST be reported on EACH APPLICABLE MEASURE in the measure set. Data collection must begin on the first day of a calendar quarter. For each measure set, circle the calendar quarter(s) for which you will report eMeasure data by 12/15/2015. 2015 CALANDAR QUARTER(s) DATA to be SUBMITTED □ AMI (AMI-7a) 1Q15 2Q15 3Q15 □ Children’s Asthma Care (CAC) 1Q15 2Q15 3Q15 □ Emergency Department (ED) 1Q15 2Q15 3Q15 □ Perinatal Care (PC) (Required if the hospital has at least 1,100 live births per year) 1Q15 2Q15 3Q15 (eAMI-7a) (Unavailable if you do not provide/rarely provide fibrinolytic therapy) (eCAC-3) (eED-1a, eED-2a) (ePC-01, ePC-05/5a) □ Stroke (STK) 1Q15 2Q15 3Q15 □ Surgical Care Improvement Project (SCIP) 1Q15 2Q15 3Q15 □ Venous Thromboembolism (VTE) 1Q15 2Q15 3Q15 (eSTK-2, eSTK-3, eSTK-4, eSTK-5, eSTK-6, eSTK-8, eSTK-10) (eSCIP-INF-1, eSCIP-INF-1-1, eSCIP-INF-1-2, eSCIP-INF-1-3, eSCIP-INF-1-4, eSCIP-INF-1-5, eSCIP-INF-1-6, eSCIP-INF-1-7, eSCIP-INF-1-8, eSCIP-INF-9) (eVTE-1, eVTE-2, eVTE-3, eVTE-4, eVTE-5, eVTE-6) NOTE: 1. For submission of 2015 discharge data, The Joint Commission will only accept data consistent with the April 2014 eCQM specifications posted on the CMS website: http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/eCQM_Library.html ). 2. A listed ORYX eMeasure Vendor’s technology must be certified by an Office of the National Coordinator for Health Information Technology Authorized Certification Body (ONC-ACB) as meeting the 2014 Edition certification criteria for calculating and submitting inpatient electronic clinical quality measures (eCQMs). 3. If your organization is seeking or is currently Joint Commission certified as a Primary Stroke Center or Comprehensive Stroke Center, data must continue to be reported on all The Joint Commission chart-abstracted Stroke measures. (Cont’d. on next page) Page 3 of 4 The Joint Commission 2015 FLEXIBLE ORYX REPORTING OPTIONS and CORE MEASURE SET SELECTION FORM SIGNATURE PAGE HCO ID# HCO NAME ADDRESS CITY, STATE, ZIP Fax Completed Forms to (630) 792-4992 Joint Commission policy requires that your organization provide written confirmation of the performance measurement system(s) and performance measures your organization has selected to meet performance measurement requirements for accreditation. Please: Review the form to be certain that you have selected a reporting option Be certain that you have indicated the measure sets on which you will be reporting data Sign the selection form below Fax the completed form to 630-792-4992 or e-mail the form to fzibrat@jointcommission.org Provide your listed core measure vendor with a copy of this form ___________________________________ __________________________________ _______________ Primary Contact Phone Date ___________________________________ __________________________________ _______________ Chief Executive Officer Signature Date Page 4 of 4 List of Chart-Abstracted Measures Measure Measure Name Label AMI-7a CAC-3 ED-1a ED-1b ED-1c ED-2a ED-2b ED-2c HBIPS-1 HBIPS-2 HBIPS-3 HBIPS-4 HBIPS-5 HBIPS-6 HBIPS-7 OP-1 OP-2 OP-3 OP-4 OP-5 OP-6 OP-7 OP-18 OP-20 OP-21 OP-23 IMM-2 PC-1 PC-2 PC-3 PC-4 PC-5/5a STK-1 STK-2 STK-3 STK-4 STK-5 STK-6 STK-8 STK-10 SUB-1 SUB-2 SUB-3 SCIPINF-4 TOB-1 TOB-2 TOB-3 VTE-1 VTE-2 VTE-3 VTE-5 VTE-6 Fibrinolytic Therapy Received Within 30 Minutes of Hospital Arrival Home Management Plan of Care (HMPC) Document Given to Patient/Caregiver Median Time from ED Arrival to ED Departure for Admitted ED Patients-Overall Rate Median Time from ED Arrival to ED Departure for Admitted ED Patients-Reporting Measure Median Time from ED Arrival to ED Departure for Admitted ED Patients- Psychiatric/Mental Health Patients Admit Decision Time to ED Departure Time for Admitted Patients-Overarll Rate Admit Decision Time to ED Departure Time for Admitted Patients-Reporting Measure Admit Decision Time to ED Departure Time for Admitted Patients-Psychiatric/Mental Health Patients Admission Screening for Violence Risk, Substance Use, Psychological Trauma History and Patient Strengths completed Hours of physical restraint use Hours of seclusion use Patients discharged on multiple antipsychotic medications Patients discharged on multiple antipsychotic medications with appropriate justification Post discharge continuing care plan created Post discharge continuing care plan transmitted to next level of care provider upon discharge Median time to fibrinolysis Fibrinolytic therapy received within 30 minutes Median time to transfer to another facility for acute coronary Intervention Aspirin at arrival Median time to ECG Timing of antibiotic prophylaxis Prophylactic antibiotic selection for surgical patients Median time from ED arrival to ED departure for discharged ED patients Door to diagnostic evaluation by a qualified medical professional ED-Median time to pain management for long bone fracture ED-Head CT scan results for acute ischemic stroke or hemorrhagic stroke who received head CT scan interpretation within 45 minutes of arrival Influenza Immunization Elective Delivery Cesarean Section Antenatal Steroids Health Care-Associated Bloodstream Infections in Newborns Exclusive Breast Milk Feeding Venous Thromboembolism (VTE) Prophylaxis Discharged on Antithrombotic Therapy Anticoagulation Therapy for Atrial Fibrillation/Flutter Thrombolytic Therapy Antithrombotic Therapy By End of Hospital Day 2 Discharged on Statin Medication Stroke Education Assessed for Rehabilitation Alcohol Use Screening Alcohol Use Brief Intervention Provided or Offered Alcohol and Other Drug Use Disorder Treatment Provided or Offered at Discharge Cardiac Surgery Patients With Controlled Postoperative Blood Glucose Tobacco Use Screening Tobacco Use Treatment Provided or Offered Tobacco Use Treatment Provided or Offered at Discharge Venous Thromboembolism Prophylaxis Intensive Care Unit Venous Thromboembolism Prophylaxis Venous Thromboembolism Patients with Anticoagulation Overlap Therapy Venous Thromboembolism Warfarin Therapy Discharge Instructions Hospital Acquired Potentially-Preventable Venous Thromboembolism List of Electronic Clinical Quality Measures (eMeasures/eCQMs) Measure Label eAMI-7a eCAC-3 eED-1a eED-1b eED-1c eED-2a eED-2b eED-2c ePC-1 ePC-5/5a eSTK-2 eSTK-3 eSTK-4 eSTK-5 eSTK-6 eSTK-8 eSTK-10 eSCIP-Inf-1 eSCIP-Inf-1-1 eSCIP-Inf-1-2 eSCIP-Inf-1-3 eSCIP-Inf-1-4 eSCIP-Inf-1-5 eSCIP-Inf-1-6 eSCIP-Inf-1-7 eSCIP-Inf-1-8 eSCIP-Inf-9 eVTE-1 eVTE-2 eVTE-3 eVTE-4 eVTE-5 eVTE-6 Measure Name Fibrinolytic Therapy Received Within 30 Minutes of Hospital Arrival Home Management Plan of Care (HMPC) Document Given to Patient/Caregiver Median Time from ED Arrival to ED Departure for Admitted ED Patients-Overall Rate Median Time from ED Arrival to ED Departure for Admitted ED Patients-Reporting Measure Median Time from ED Arrival to ED Departure for Admitted ED Patients- Psychiatric/Mental Health Patients Admit Decision Time to ED Departure Time for Admitted Patients-Overarll Rate Admit Decision Time to ED Departure Time for Admitted Patients-Reporting Measure Admit Decision Time to ED Departure Time for Admitted Patients-Psychiatric/Mental Health Patients Elective Delivery Exclusive Breast Milk Feeding Discharged on Antithrombotic Therapy Anticoagulation Therapy for Atrial Fibrillation/Flutter Thrombolytic Therapy Antithrombotic Therapy By End of Hospital Day 2 Discharged on Statin Medication Stroke Education Assessed for Rehabilitation Prophylactic Antibiotic Received Within One Hour Prior to Surgical Incision - Overall Rate Prophylactic Antibiotic Received Within One Hour Prior to Surgical Incision - CABG Prophylactic Antibiotic Received Within One Hour Prior to Surgical Incision - Other Cardiac Surgery Prophylactic Antibiotic Received Within One Hour Prior to Surgical Incision - Hip Arthroplasty Prophylactic Antibiotic Received Within One Hour Prior to Surgical Incision - Knee Arthroplasty Prophylactic Antibiotic Received Within One Hour Prior to Surgical Incision - Colon Surgery Prophylactic Antibiotic Received Within One Hour Prior to Surgical Incision – Abdominal Hysterectomy Prophylactic Antibiotic Received Within One Hour Prior to Surgical Incision - Vaginal Hysterectomy Prophylactic Antibiotic Received Within One Hour Prior to Surgical Incision - Vascular Surgery Urinary catheter removed on Postoperative Day 1 (POD 1) or Postoperative Day 2 (POD 2) with day of surgery being day zero Venous Thromboembolism Prophylaxis Intensive Care Unit Venous Thromboembolism Prophylaxis Venous Thromboembolism Patients with Anticoagulation Overlap Therapy Venous Thromboembolism Patients Receiving Unfractionated Heparin with Dosages/Platelet Count Monitoring by Protocol or Nomogram Venous Thromboembolism Warfarin Therapy Discharge Instructions Hospital Acquired Potentially-Preventable Venous Thromboembolism