- Royal College of Paediatrics and Child Health
advertisement

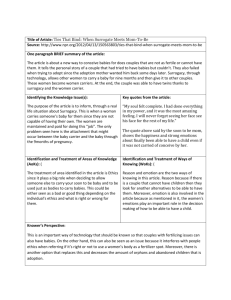
Neonatal Feeding and Fluid Guideline Jinja Regional Referral Hospital Background The incidence of LBW is 14.3% in Africa, with little variation across the region as a whole. When babies are small or born preterm, there is an increased risk of feeding difficulties for the newborn. This can be due to immature/ absent sucking reflexes in the baby or secondary to many neonatal conditions including infections and congenital abnormalities. This guideline is attended for use by healthcare staff caring for neonates at Jinja Regional Referral Hospital; it is not intended for wider distribution to other healthcare facilities where the ability to follow these guidelines may be restricted. Introduction There is strong and consistent evidence that feeding mother’s own milk to pre-term infants of any gestation is associated with a lower incidence of infections and necrotising enterocolitis, as well as improved neurodevelopmental outcome as compared with formula feeding. When giving feeding advice to a mother about her baby, it is important that exclusive breastfeeding for the first six months of the child’s life is advocated wherever possible, in accordance with the WHO advice. What to do when there is no/ reduced breast milk supply Supporting and educating the mother about breastfeeding is the best way to ensure that the mother’s milk supply is optimal for the baby’s nutritional requirements. Health workers should be able to explain and demonstrate good breast-feeding positions in order to help establish breastfeeding as early as possible (see figure below). • Baby's whole body toward mother • Chest to chest • Touch baby’s upper lip with nipple, when opens mouth wide, pull baby onto the breast • Holding breast for support Morgan, J. 2013 1 • Mouth should cover not just the nipple but as much of the areola (the darker part surrounding it) as possible Figure 1. Attachment of baby at mother’s breast Short term feeding alternatives include cup feeding expressed breast milk or inserting a nasogastric tube. If alternative feeding methods are used, mothers should be encouraged to continue to spend as much time as possible with their baby, ideally in the Kangaroo care position in order to facilitate bonding and stimulate mother’s milk supply. If babies are <1.0 kg at birth, they will not be able to suck effectively enough to get an adequate supply of milk. These babies should have an NG tube inserted when feeding is due to start in order to ensure that they get adequate nutrition (please see appendix on ‘How to insert an NG tube’). Babies <1.5kg are also more likely to experience feeding difficulties and should have a graduated introduction of milk. You MUST ensure that the mother’s nutritional intake is adequate enough to produce a good supply of breast milk. A mother that is malnourished will not be able to produce enough breastmilk and both the baby and the mother’s health will be at risk. Traffic lights system All babies can be categorised into green, yellow or red groups. When a neonate is admitted to special care unit, please ensure they are placed into correct feeding plan as per this guideline. Green Morgan, J. 2013 2 - Birth weight >1.5kg No evidence significant infection No congenital abnormalities identified No delayed passage of meconium (if known) No vomiting or per rectal blood. Breastfeed as normal or give expressed breast milk by cup at daily requirements. No iv fluids required unless feeding fails. Yellow - Birth weight 1.0-1.5kg or >1.5kg with significant infection Known antenatal absent/reversed end-diastolic flow Milky vomiting ONLY Do not feed for at least first 24 hours. Give 10% dextrose at 60ml/kg/day, then 80ml/kg/day on day 2 if required. Electrolytes need to be added to fluids from day 3 onwards. Gradual introduction of feeds following initial period of intravenous fluids only as per figure C (feed requirements for VLBW infants). Red - Birth weight <1.0kg Bilious vomiting Delayed passage of meconium Per rectal bleeding Abdominal distension with visible bowel loops/ colour change DO NOT FEED for 48 hours. Begin feeding at 24ml/kg/day, then 48ml/kg/day, then 72 ml/kg/day, then 96ml/kg/day, then 120ml/kg/day, then 150ml/kg/day, then 165ml/kg/day, then 180ml/kg day. Day 1- no feed, iv 10% dextrose only at 60ml/kg/day Day 2- no feed, iv 10% dextrose only at 80ml/kg/day Day 3- EBM 24ml/kg/day + remainder of fluids (76ml/kg/day) as iv 10% dextrose and ringers lactate Day 4- 48ml/kg/day Day 5- 72ml/kg/day Day 6- 96ml/kg/day Morgan, J. 2013 3 Day 7- 120ml/kg/day Day 8- 150ml/kg/ day Day 9- 165ml/kg/day Day 10- 180ml/kg/day Initiate appropriate antibiotic coverage if bowel obstruction or necrotising enterocolitis suspected (ampicillin, gentamicin and metronidazole). Remember to insert an NG tube and place on free drainage to relieve intra-abdominal pressure if bowel obstruction or NEC (necrotising entercolitis) suspected. Feed requirement Term babies and babies >1.5kg weight should initiate breastfeeding as soon as possible, providing they are not unwell. Babies should gain about 10g / kg of body weight every day after the first 7 days of life. If they are not, check that the right amount of feed is being given. Weight should be checked on admission, then at 3 days, 5 days, 7 days and twice weekly thereafter. Normal birthweight = > 2.5kg Low birth weight = 1.5- 2.5kg Very low birthweight = 1.0- 1.5 kg Extremely low birthweight = <1.0 kg If there are any concerns about the hydration status of the baby i.e. very sick, appears dehydrated or suspected cardiac failure (heart murmur, peripheral oedema, oxygen requirement, tachypnoea) then weigh baby DAILY. Morgan, J. 2013 4 When to start feeds For babies with a birth weight > 1.5kg, without any congenital anomalies, breastfeeding should be initiated as soon as possible. Babies in the ‘red’ category i.e. birth weight less than 1.0kg should not receive feeds for the first 48 hours following delivery; they should be started on intravenous 10% dextrose Which fluid to use Figure 2. Composition of intravenous fluids (per L) Morgan, J. 2013 5 10% dextrose Given to babies that are at risk of hypoglycaemia and used for those requiring maintenance fluids in the first 48 hours of life. Babies should NOT be given fluids containing electrolytes in the first 48 hours. Ringer’s Lactate Given to babies for rehydration and help with maintaining normal electrolytes. Contains sodium and potassium and best used in combination with some 10% dextrose if on IV fluids from day 3 of life. ½ DS (Darrow’s solution) Contains half the sodium and twice the potassium of ringer’s lactate. Can be used in combination with 10% dextrose to maintain normal electrolytes in babies from day 3 of life. Normal saline Can be given to babies requiring resuscitation or to replace losses from abnormal bowels e.g. gastroschisis or exomphalos. It should not be used for maintaining the fluid requirements of babies that are not feeding as it contains too much sodium. 25% and 50% dextrose Morgan, J. 2013 6 Should NEVER be given to neonates. If you are concerned that a baby is hypoglycaemic, give 5ml/kg of dextrose 10% Rehydration of dehydrated newborns Newborns can get dehydrated quickly if adequate feed or fluids are not administered. However, it can be normal for term babies of normal birth weight (>2.5kg) to take up to 72 hours to establish breastfeeding. If the baby is passing urine and stool regularly and does not appear clinically dehydrated or lethargic- there is no indication to give intravenous fluids. Signs of dehydration in newborns 1) 2) 3) 4) 5) 6) Decreased urine output Weight loss Prolonged skin pinch Dry mucous membranes Sleepy or unable to feed Sunken fontanelle Treating dehydration Weigh the baby- this is the most accurate assessment of dehydration in a newborn due to their high water content. Give up to 20ml/kg as a fluid bolus for severe dehydration and ensure that hypoglycaemia is corrected. Fluid regimes after day 3 of life should include some attempt to correct electrolyte imbalances as well as maintain normal glucose levels. Aim to correct their dehydration slowly over the next 48 hours. The best way to rehydrate a baby is using mother’s breast milk. If possible, monitor the serum electrolytes. HOW TO CALCULATE FLUID REQUIREMENTS Age of baby (days), then refer to table re: feeding requirements on day 1-7 life. Number of ml/kg required x birth weight = total number of mls of fluid/ day (24 hours) Morgan, J. 2013 7 To calculate the number of mls required at each feed, divide the total number of mls of fluid required in 24 hours by 12 (to get 2 hourly feed amounts) OR by 8 (to get 3 hourly feed amounts). Example 1.4 kg baby- requires iv maintenance fluids from birth. Should receive 60ml/kg/day for day 1. Will require 10% dextrose only. 60 x 1.4 = 84 mls 84 mls fluid needed in 24 hours, plan for 2 hourly feeds. 84/12 = 7 mls fluid required every 2 hours (see prescription below). Always record how much fluid has been given to a baby and sign the chart, writing the date and time fluid was given. Babies can become overloaded and oedematous if too much fluid is given, the child is septic or the child has an underlying cardiac condition. Signs of fluid overload - Excessive weight gain Periorbital or genital oedema Oxygen requirement Tachypnoea Harsh sounding heart murmur If you are concerned that a baby is fluid overloaded or has signs of cardiac failure, ensure that fluids are appropriately reduced and consider the use of a diuretic (1mg/kg of furosemide iv or po). Ideally, their renal function should be tested. When reducing fluids, ensure that the baby is monitored closely for signs of hypoglycaemia. Hypoglycaemia Morgan, J. 2013 8 Hypoglycaemia in the newborn is defined as a blood glucose of < 2.6mmol/L. Babies that do not feed are at risk of hypoglycaemia and if there is any concern that a baby is hypoglycaemic, treatment should be given. If you do not have a glucometer to measure the blood glucose, there are some clinical signs that you can look for in order to determine if a baby has a low blood sugar. These include: - sleepiness or lethargy convulsions jitters (shaking movements of arms and legs that stop when you hold affected limb) High risk babies include - Preterm babies Infant of a diabetic mother Babies with severe sepsis/ meningitis Treatment options include a) immediate feed (breast/cup/NG) b) 5ml/kg bolus of iv 10% dextrose Be aware that treating with dextrose once is unlikely to fix the feeding difficulties immediately, therefore a clear feed and fluid plan should be made for the next few hours after treating hypoglycaemia, to ensure it does not recur. Vitamins and Mineral Supplementation All preterm and low birth weight babies should receive nutritional supplementation with Grovit drops 0.3ml once daily for at least 14 days. Each 0.3ml Grovit contains 2500iu vitamin A, 200iu vitamin D, vitamin B1 0.5mg, Vitamin B2 0.2mg, vitamin C 25mg, nicotinamide 2.5mg. Ferrous fumurate (sytron) supplementation should start from 8 weeks age for the next 12 weeks in any baby that is preterm or has a birth weight <2kg. Dose = 2.5ml once daily. SPECIAL CIRCUMSTANCES A) Necrotising Enterocolitis If a baby develops bilious vomiting, significant abdominal distension or passes blood per rectumSTOP FEEDS IMMEDIATELY. This baby may have NEC (necrotising enterocolitis). Feeds should be stopped for at least 48 hours, with clear explanation to the mother about the concerns. Insert an NG tube and allow free drainage of abdominal contents. Morgan, J. 2013 9 Arrange an abdominal x-ray- look for signs of intramural gas, thickened bowel loops or intestinal perforation. Treat the baby with triple intravenous antibiotics: ampicillin, gentamicin and metronidazole Consider treating with iv vitamin K 1mg if blood per rectum. B) SURGICAL PROBLEMS Cleft lip & palate Babies with an isolated cleft lip should be able to breastfeed normally. The baby should be offered an early breastfeed straight away. Babies with cleft palates can sometimes struggle to breast feed and may need to use alternative methods. Mothers should express breast milk and feed the child with a cup and spoon. This should be tried cautiously under supervision from nursing or midwifery staff, to ensure the baby does not choke or aspirate milk. Mothers should be advised that the baby should sleep on it’s side with a rolled up blanket behind the back in order to prevent accidental aspiration whilst sleeping. Early referral to a centre that can assess the defect for repair is essential i.e. Mbale Regional Referral Hospital or Mulago Hospital, Kampala. Imperforate anus/ meconium ileus Most newborn babies will pass meconium within 24 hours of birth and all should pass meconium within 48 hours of delivery. If the passage of meconium is delayed, there may be a structural bowel abnormality or an obstruction to the passage of meconium within the bowel. It is important to check that the position of the anus is normal and that the anus is not imperforate in any child with a history of delayed passage of meconium. If the anus appears normal, an urgent abdominal x-ray should be arranged for the baby and feeding withheld until any structural problems have been ruled out. Exomphalos/ gastroschisis The feeding and fluid management for these babies is often very difficult, due to the large amount of fluid being lost to the atmosphere through the exposed bowel wall. Babies who are born with these congenital abnormalities of the bowel require early assessment by the surgical team. While awaiting the surgeon’s review, do not feed the baby. Insert an intravenous cannula and give 10% dextrose fluid at normal requirements + an extra 30ml/kg/day of 0.9% saline, to account for the fluid lost through the exposed bowel wall. Morgan, J. 2013 10 Insert an NG tube to allow the stomach contents to drain freely and avoid additional pressure on the abnormal bowel. Babies with severe infection Babies with severe infections may not tolerate normal feed volumes if if their gut has no structural abnormality. Fighting an infection can lead to reduced gut motility and vomiting, if large volumes of feed are used. This intolerance to feed will improve as the infection is treated, but the baby may require smaller volumes of feed for a few days. If this is the case, ensure that intravenous fluids are used to achieve daily fluid requirements as necessary. C) Babies born to mothers with HIV Mothers that are HIV positive during pregnancy should be advised to exclusively breast feed their babies. The baby should only be offered formula feeding at birth if the supply of baby formula can be maintained throughout infancy and is AFASS (acceptable, feasible, affordable, sustainable, safe). For most women delivering at Jinja hospital, this will not be the case. It is very important to ensure that the mother does not mix feed (i.e. some formula and some breastmilk) as this has been shown to have an increased risk of transmission of HIV to the baby. Ensure that no other milk substitutes are given e.g. cow’s milk, as they are deficient in iron and can affect the neurological development of the baby long-term. References 1) 2) 3) 4) 5) Basic paediatric protocols- Kenyan guidelines, revised 2010 Optimal feeding of low-birth-weight infants. Technical review, WHO Nottingham Neonatal Service guidelines WHO, pocketbook of Hospital Care for Children, 2009. Nutritional Unit, Jinja Regional Referral Hospital Morgan, J. 2013 11 APPENDIX 1: Neonatal Fluid Chart Morgan, J. 2013 12 APPENDIX 2: Insertion of a nasogastric (NG) tube 1. Select the correct size NG tube (babies will require between a 3Fr and 5Fr size NGT to fit comfortably). 2. Holding the tip against the child’s nose, measure the distance from the nose to the earlobe, then to the xiphisternum (epigastrium). Mark the tube at this point. 3. Hold the baby firmly. Lubricate the tip with water and pass directly down one nostril. The nasal cavity travels straight backwards before curving down towards the baby’s body, so aim the NG tube directly backwards from the nose initially when inserting. 4. When the measured distance is reached, secure with tape. 5. Aspirate a small amount of fluid to ensure that the tube is in the correct place. If there is any doubt over the position of the NG tube, remove it and start again. Baby’s will often cough or sneeze as the NG tube is being inserted but should not change colour. If the colour changes during insertion of the NG tube, remove it immediately. Picture taken from WHO Hospital Care for Sick Children pocketbook, 2009. Morgan, J. 2013 13 Appendix 3: Flow chart of feeds Birth weight? <1kg 1.0-1.5kg >1.5kg Baby clinically well? Baby clinically well? Baby clinically well? No Yes Yes No No Features of NEC or bowel obstruction? Features of NEC or bowel obstruction? Yes Yes Yes No No Persistent milky vomiting or feed intolerance, without features of NEC RED regime + arrange xray abdomen, triple antibiotics and NGT Yes Follow RED regime Morgan, J. 2013 Follow YELLOW regime Follow RED regime Follow YELLOW regime No Breastfeed or EBM at daily requirements GREEN 14