40258_2014_109_MOESM1_ESM
advertisement

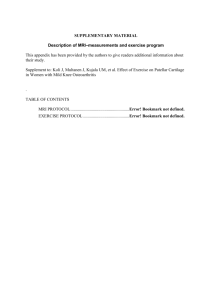
Appendix 1: Summary of Visionscope Imaging System (VSI) versus MRI plus clinical workup Materials & Methodology: A prospective multicenter study was performed of all patients who had a routine surgical arthroscopy at one of the six participating clinical sites between July 2012 and May 2013. Patients were consented by the physician investigator at each site. Study inclusion criteria consisted of suspected meniscal tears or articular cartilage damage. Patients were excluded from the study if they had (1) acute traumatic hemarthoses, (2) concomitant ligament injury, (3) active systemic infection, (4) allergy to silicone or any medication used during the procedure, (5) enrollment in another pharmacological or medical device study, (6) institutionalized persons, prisoners and persons with decisional incapacity, or (7) investigators own students and employees. All patients had a MRI and a comprehensive physical exam prior to their surgical arthroscopy. Patients were identified based on presentation of knee symptoms including effusion, popping, locking and were prescribed a pre-operative diagnostic MRI for the purpose of determining whether arthroscopic surgery may be necessary. Subjects were otherwise in good health based on their medical history and physical examination. Prior to each arthroscopy, physicians performed a VSI procedure. Surgeons were asked to record and capture images during the VSI procedure on a standardized data collection form. After the completion of the VSI procedure, a standard surgical arthroscopy was performed. During the standard arthroscopy, Surgeon’s were asked to capture images and video. Each was asked to provide a copy of the MR images, a completed arthroscopy case report form [CRF], a completed VSI CRF, diagnostic arthroscopy images and VSI images. 1 The VSI and MRI images were reviewed by two blinded experts, an orthopedic surgeon unaffiliated with the study sites and a musculoskeletal radiologist. These experts were blinded to radiological readings and surgical notes. In addition, the images were reviewed in a randomized order with separate readings. The diagnostic arthroscopy served as the gold standard for comparison between the VSI and MRI images. Analyses were performed separately for the Surgeon’s assessments, and the blinded reader’s assessments. It was not considered appropriate to compare a blinded reader’s assessment of an MRI, to the Surgeon’s assessment of arthroscopy, since the quality of the images for the two could be quite different. Therefore, all analyses were done twice, once using Surgeon’s assessments, and once using the Blinded Reader’s assessments. The primary comparisons with MRI were with the Blinded Reader assessments. The primary comparisons for VSI versus arthroscopy were done with the Surgeon’s assessments [i.e. the Surgeon who had performed the actual VSI and surgical arthroscopy] (based on CRFs). Statistical analysis All statistical analysis was completed by the author (JV). Comparisons were made using the Cochrane Review statistical packages for diagnostic test[1] and included: risk ratios (probability of an incorrect event [a FP or FN] with VSI versus MRI; or the relative risk reduction in an incorrect event with one diagnostic versus another) (Table 1); sensitivity, specificity and accuracy analysis (Table 2); and receiver operating characteristic (ROC) curves (Figures 1-6). ROC curves are a graph of the sensitivity versus the specificity. The best possible diagnostic result (when compared to the gold standard of surgical 2 arthroscopy) would yield a point in the upper left corner or coordinate (1,1) of the ROC space, representing 100% sensitivity (no false negatives) and 100% specificity (no false positives). Table 1: Risk ratios Comparison Medial meniscal tears Risk ratio RR =0.19; 95% CI [0.07-0.47] P value P = 0.0003 Lateral meniscus tears RR = 0.41; 95% CI [0.19-0.90] P =0.03 Medial tibial articular cartilage tears RR = 0.18; 95% CI [0.08-0.41] P<0.0001 Lateral tibial articular cartilage tears RR = 0.25; 95% CI [0.13-0.47] P<0.0001 Medial femoral articular cartilage tears RR = 0.21; 95% CI [0.08-0.53] P=0.001 Lateral femoral articular cartilage tears RR = 0.31; 95% CI [0.48-1.50] P=0.002 3 Interpretation Using VSI results in a 73% lower risk/chance of obtaining an incorrect result vs. MRI; Using VSI results in a 59% lower risk/chance of obtaining an incorrect result; Using VSI results in an 82% lower risk/chance of obtaining an incorrect result; Using VSI results in a 75% lower risk/chance of obtaining an incorrect result; Using VSI results in a 79% lower risk/chance of obtaining an incorrect result; Using VSI results in a 69% lower risk/chance of obtaining an incorrect result Table 2: Sensitivities, Specificities, Accuracy of VSI and MRI compared to standard arthroscopy (gold standard) – study data (community setting) Comparison Medial meniscal tears Lateral meniscus tears Medial tibial articular cartilage tears Lateral tibial articular cartilage tears Medial femoral articular cartilage tears Lateral femoral articular cartilage tears VSI Sensitivity 94% MRI Sensitivity 81% VSI Specificity 97% MRI Specificity 61% Accuracy VSI 94% (n=103) Accuracy MRI 74% (n=100) 90% 67% 93% 87% 92% (n=100) 80.6% (n=98) 88% 41% 96% 90% 94% (n=94) 65% (n=97) 83% 39% 96% 86% 89.2% (n=93) 61% (n=93) 96% 85% 94% 66% 95% (n=102) 77% (n=99) 82% 58% 95% 85% 92% (n=99) 74% (n=95) Table 3: Sensitivities, Specificities, Accuracy of VSI and MRI compared to standard arthroscopy (gold standard) – systematic review data (academic setting) [2] Comparison Medial meniscal tears Lateral meniscus tears VSI Sensitivity 94% MRI Sensitivity 91% VSI Specificity 97% MRI Specificity 81% Accuracy VSI 94% Accuracy MRI 86% 90% 76% 93% 93% 92% 89% 4 Figure 1: ROC curve Medial Meniscus Tears 5 Figure 2: ROC curve lateral meniscus tears 6 Figure 3: ROC curve medial tibial articular cartilage tear 7 Figure 4: ROC curve lateral tibia articular cartilage tears 8 Figure 5: ROC curve medial femoral articular cartilage tears 9 Figure 6: ROC curve lateral femoral articular cartilage tears 10 References: 1 Higgins JPT, Green S. (editors). Cochrane Handbook of Systematic Reviews and interventions. Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochranehandbook.org. 2 Crawford R, Walley G, Bridgan S, Maffuli N. Magnetic resonance imaging versus arthroscopy in the diagnosis of knee pathology, concentrating on meniscal lesions and ACL tears: a systematic review. Br Med Bull. 2007;84:5-23. 11