Super-User Practice Scenario Name: Unit: Date: ¶ Highlighted
advertisement

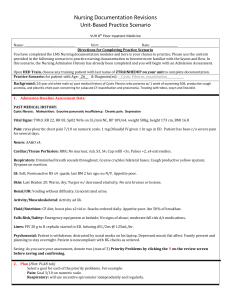
Super-User Practice Scenario Name: ____________________ Date: ___________________ Unit: ______________ Highlighted portions indicate where Educators will need to customize scenario to their patient population. Directions for Completing Practice Scenario Please use the content provided in the following scenario to practice nursing documentation to become more familiar with the layout and flow. In this scenario, the Nursing Admission History has already been completed and you will begin with an Admission Assessment. Open HED Train, choose any training patient with last name of ZTRAINHEDUP on your unit to complete documentation. Practice Scenario: for patient with Age: _58_ & Diagnosis(es): _Idiopathic Liver Failure__ Background: Educator to tailor scenario to common patient population of the unit. Example: This is a 58 year previously healthy Caucasian female who presents with altered mental status, nausea, no vomiting, and abdominal swelling. Liver enzymes elevated. Smoked 1 pack per day x 20 years (quit 6 years ago). Denies ETOH. 1. Admission Baseline Assessment Data: PAST MEDICAL HISTORY: Examples: - Hypertension - Diabetes - COPD w/ home O2 - MVC w/ injury L arm 2 yrs ago PAST SURGICAL HISTORY: - C-section Vital Signs (T,P,R, BP, Pulse Ox, Pain score): 98.9, 134, 20, 135/90, 96% on 3L/min Pain: rates RUQ abd pain 3/10 on numeric scale. 0.5mg Dilaudid IV given 1 hr ago in ED. Neuro: Drowsy. Awakens to verbal stimuli. Disoriented to time. No asterixis. Cardiac/Tissue Perfusion: RRR, cap refill <3s, no abnormal sounds. Pulses +3, x4 extremeties. BLE moderate edema Respiratory: Clear, BL breath sounds, moving air well GI: soft, tender RUQ, distended; hyperactive bowel sounds; last BM 1 day ago; nausea, no vomiting Skin: warm, dry; normal turgor, no cuts bruises or lesions. Jaundiced. Renal/GU: Voiding without difficulty. Urine tea colored. Activity/Musculoskeletal: Residual L-arm weakness s/p injury 2 yrs ago, +3 LUE; moves all extremities, pink, warm, Super-User Practice Scenario Fluid/Nutrition: NPO since midnight. Falls Risk/Safety: slip resistant socks on, emergency equipment at bedside, no signs of abuse Lines: PIV 18G to R cephalic started in ED. Infusing d51/2ns @ 75mL/hr. Psychosocial: Family present and planning to stay overnight. Appropriate interactions. Medication: Polypharmacy Lines: Left, cephalic 18G, PIV; transparent drsg, dry intact, w/ biopatch; site dry, warm. Self-Care: WNL Infection/Metabolic: Infection risk d/t impaired liver function 2. Priority Problems and Goals: (Hint: PLAN tab) Upon completing assessment, will need to denote two Priority Problems and set goals for each. 1. Neurological: AAOx4: person, place, time, & situation. 2. Safety/Fall: (Annotate) Pt will call for assistance up OOB. 3. Nursing Interventions: Document the following interventions (Hint: Interventions tab) Neuro: Reoriented to time Vascular/Perfusion: Extremities elevated, compression wrap Activity/Musculoskeletal: Assist x1 to chair. 4. Re-Assessment: You have just performed a focused re-assessment. Document the following: Re-assessment reveals the following changes. Therefore, denote unchanged except. (There would not typically be data in all of these categories). Pain: Neuro: Awakens to verbal stimuli. Disoriented time & place. Cardiac/Tissue Perfusion: Tachycardic, HR 135. Respiratory: GI: Skin: Renal/UR: Activity/Musculoskeletal: Fluid/Nutrition: Falls Risk/Safety: Lines: Psychosocial: Super-User Practice Scenario 5. End of Shift: It is now the end of your shift. Document the following: Response to Care/Recommendations: Worsening mental status despite lactulose; continue lactulose. Neuro checks q2h. Patient education (Hint: EDUCATION tab) Upon completion, please sign and return to Nursing Educator by Print Name: Signature: Date: DATE .