Massive transfusion Definition >50% patient`s blood vol at once or
advertisement

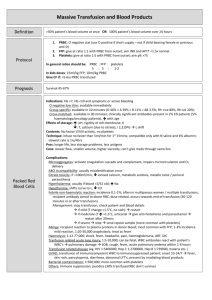
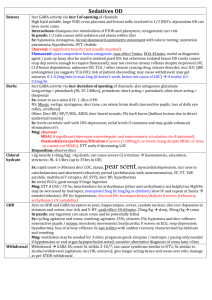
Definition Mng Massive transfusion >50% patient’s blood vol at once or 100% patient’s blood vol over 24hrs 1. PRBC: O neg stat (use O pos if short supply – not if child-bearing female or prev anti-D) 2. FFP: give 1:1 with PRBC from outset; aim INR and APTT <1.5x normal 3. Plt: give 1:5 with PRBC from outset; aim plt >75 PRBC : FFP : plt 5 : 5 : 1-2 Give CF if >5-6iu transfused In kids doses: 15ml/kg FFP; 10ml/kg PRBC Outcome PRBC Survival 45-67% Indications: Hb <7, Hb <10 and symptoms or active bleeding O neg low titre: immediate Group specific: 10mins; O 46% > A 39% > B 11% > AB 3.5%; Rh +ive 80%, Rh-ive 20% XM: 30mins; clinically significant ab’s present in 2% ED patients (5% haem/onc patients), incr with age Effects of storage: incr pH, decr T, decr Ca (due to citrate), incr rigidity of cell membrane, hyperK, decr 2,3,DPG L shift, no factor V/VIII activity, no plts Technique: infuse no faster than 5ml/min for 1st 15mins; compatible only with N saline and 4% alb; slowest rate is 1iu/4hrs Pros: longer life, less storage problems, less Ags Cons: slower flow, smaller vol, higher viscosity; can’t give meds through same line Complications: Microaggregates (activate coagulation cascade and complement, impairs microcirculation and O2 delivery) ABO incompatibility (usually misidentification error) Citrate toxicity (if >100ml/min; decr ionised Ca, metabolic acidosis, metallic taste / perioral paraesthesia) HyperK (usually if blood >2/52 old); hyperNa Hypothermia (shifts curve to L, decr CO) Febrile non-haemolytic reaction (incidence 0.1-1%; often in multip/multiple transfusions; recipient ab to donor RBC; dose related, towards end of transfusion 30-120mins in or after transfusion; stop transfusion, check pt and blood details if mild (T change <1.5, no rash), restart / if mod (T incr >1.5, urticaria), give anti-histamines and paracetamol, restart after 20mins / if severe stop, send rpt sample; more common with plts) Allergy (recipient reaction to pp’s in donor blood; most common with FFP; 1-3% incidence mild reaction, 1:2050,000 anaphylaxis; trt as fever) Haemolysis (1:12-77,000; shock, fever, headache, pain, Hburia, ARF, DIC) Tranfusion related acute lung inj (1:5-10,000; can be fatal; WBC ab’s react with patient’s WBC’s pul damage SOB, cough, fever, APO within 1-6hrs) Bacterial contamination (1:500,000; more common with plt) Immune suppression; jaundice (30% transfused RBC don’t survive) Transfusion related disease (eg. HIV 1:5400000, Hep C 1:2700000, Hep B 1:739000, malaria etc..) GVHD (transfusion of immunocompetent WBC to immunosupp patient; onset 10-14/7 fever, skin rash, pancytopenia, diarrhoea, abnormal LFT’s; prevent by irradiating blood products) FFP Available in ; do require ABO compatibility; contains all CF’s + fibrinogen; give at 10ml/min (ie over <1hr); give 4-6iu per 5L blood Indications: haemorrhage and coagulopathy; reversal of warfarin OD; factor def; AT III def; TTP; can be used in Haemophilia A and B in emergency if no pure factor available (although risk of vol overload) Cryo Available in ; better if ABO compatibility; contains VIII/XIII, fibrinogen, vWF; give at 10ml/min (ie over <1hr); give 1iu / 10kg body weight ; no factor 9, so can be used in Haemophilia A but not B in emergencies (although would be risk of fluid overload in amounts required) Indications: bleeding and fib <1 Plt Available in ; do not require ABO compatibility; can only be stored 3/7; 1iu incr plt 5; give 12 units per 5L blood Indications: plt <10 <20 and fever / antibiotics / evidence of systemic haemostatic failure <50 and bleeding (or skin bleeding time >2x normal) or OT <100 and for eye / neuro OT 30mins 30mins 15-30mins DIC / ITP with life-threatening haemorrhage PTX Factor VIIa Contains II/V/VII/IX/X, anti-thrombin and heparin; DOA 12-24hrs; give 3ml/min; give 25-50iu/kg (50iu if INR >6, 35iu if INR 4-6, 25iu if INR 2-4) Indications: congenital CF def, warfarin OD and significant bleeding Pros: small vol, rapid admin, no time delay in thawing (unlike FFP), no ABO typing (unlike FFP), INR reversal within 15mins, no disease transmission Not demonstrated to improve any clinically significant outcomes in trials; incr mortality in blunt trauma in CONTROL trial, expensive, requires normal pH and T to be effective; 5% absolute incr risk of VTE; give 90-120mcg/kg Indications: last resort in generalised bleeding only after control of bleeding obtained; inhibitors to CF VIII/X; congenital CF VII def; Glanzmann’s thrombasthenia Notes from: Dunn