LEAP School Visit Checklist - Louisiana Department of Education
advertisement

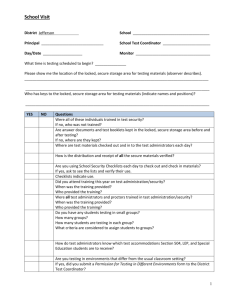
School Visit Checklist District ________________________________ School __________________________________________ Principal ______________________________ School Test Coordinator ___________________________ Day/Date ___________________ Observer ________________________________________ What time is testing scheduled to begin? _______________ Please show me the location of the locked, secure storage area for testing materials (observer describes). _________________________________________________________________________________________ _________________________________________________________________________________________ _________________________________________________________________________________________ Who has keys to the locked, secure storage area for testing materials (indicate names and positions)? _________________________________________________________________________________________ Were all of these individuals trained in test security? Yes No If no, who was not trained? ____________________________________________________________ Are answer documents and test booklets kept in the locked, secure storage area before and after testing? Yes No If no, where are they kept? ___________________________________________ Where are test materials checked out and in to the test administrators each day? _________________________ _________________________________________________________________________________________ How is the distribution and receipt of all the secure materials verified? _________________________________ __________________________________________________________________________________________ Are you using School Security Checklists each day to check out and check in materials? (If yes, ask to see the lists and verify their use.) Yes No Checklists indicate use: Yes No Describe the procedure for students who need additional time to finish any session of the test (including where they test and how materials are kept secure). _________________________________________________________________________________________ _________________________________________________________________________________________ _________________________________________________________________________________________ OVER Did you attend training this year on test administration/security? Yes No When was the training provided? _______________ Who provided the training? __________________ Were all test administrators and proctors trained in test administration/security? Yes No When was the training provided? _______________ Who provided the training? __________________ How do test administrators know which test accommodations Section 504, LEP, and Special Education students are to receive? __________________________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ Do you have any students testing in small groups? _________ How many groups? _________ How many students are testing in each group? __________ What criteria are considered to assign students to groups? __________________________________________________________________________________________ __________________________________________________________________________________________ Describe the procedure for removing all test materials from the classroom during an extended break and after testing is completed each day. __________________________________________________________________________________________ __________________________________________________________________________________________ Describe the procedure for the administration of makeups (including where test materials will be stored, where students will take the test, who will administer the makeups, security procedures, etc.). __________________________________________________________________________________________ __________________________________________________________________________________________ Are you testing in environments that differ from the usual classroom setting? Yes No If yes, did you submit a Permission for Testing in Different Environments form to the District Test Coordinator? Yes No Classroom Observation Day/Date ____________ District ________________________ School ______________________________ Test Administrator ____________________________ Observer ___________________________________ Number of Students in Room _____________ Circle Test: Yes Number of Proctors in Room ___________ LEAP Grade______ GEE ELA Math Science Social Studies LAA 2 ELA Math Science Social Studies No ELA Math Students were seated with sufficient space between them. ________________________________________________________________ Yes No Students had room for materials and to write at desks or tables. ________________________________________________________________ Yes No Classroom is prepared for testing (content-related bulletin boards or posters covered or removed, testing sign on door). ________________________________________________________________ Yes No The test administrator disseminated and picked up test booklets and answer documents in a systematic order. ________________________________________________________________ Yes No The test administrator read directions as written. ________________________________________________________________ Yes No The test administrator disseminated and picked up test materials (dictionaries, thesauruses, Writer’s Checklists, calculators, Mathematics Reference Sheets, etc.) as directed in the Test Administration Manual. ________________________________________________________________ Yes No The test administrator carefully monitored students during testing. ________________________________________________________________ Yes No Directions or interruptions disturbed testing. ________________________________________________________________ OVER Test Administrator Questions Did you attend training on test security and administration procedures this year for this test administration? Yes No If yes, who provided this training? _______________________________________________________ Did you receive your Test Administration Manual prior to the day of testing? Yes No Have you reviewed the Oath of Security and Confidentiality Statement? Yes No Do any students in your testing group receive accommodations? Yes No If yes, how do you know what accommodations they need? ____________________________________ ___________________________________________________________________________________ Did your students ask any questions during testing? Yes No If yes, what was the nature of these questions? _____________________________________________ ___________________________________________________________________________________ _____________________________________________________________________________ What arrangements have been made for students who need additional time to complete testing? __________________________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ What do you do if you observe any testing irregularities including possible cheating? __________________________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ Do you have any other comments? __________________________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ Additional Observation Notes Day/Date _________________ District __________________________ School ______________________ School Test Coordinator _______________________ Test Administrator ___________________________ Observer ____________________________________ Describe any testing irregularities. Please note any other observations.