NervousSystem6
advertisement

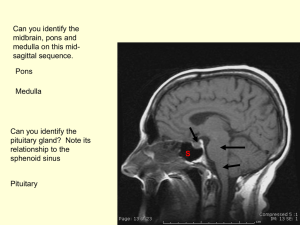
Cranial nerves III, IV, and VI (a brief summary is at the end of this presentation): General. Cranial nerves III, IV, and VI, innervate the extraocular muscles. The extraocular muscles are the striated muscles that attach external to the eyeball. They are to be differentiated from the intraocular muscles, which, in our domestic mammals, are smooth muscle and internal to the eyeball. The innervation of the ocular muscles is significant in examining the animal as “eye movement and the resting position of the eyes; and appearance of the pupil” are three of the clues that we use routinely. See the list at the end of Nervous System 2. The third cranial nerve is the oculomotor (eye-motor) nerve; the fourth is the trochlear nerve, named after the pulley-like (trochlear) arrangement of its tendon with the trochlear cartilage: and the sixth is the abducent nerve, named according to its abducting action in turning the eyeball so that the gaze is lateral. In addition to muscles that move the eyeball, the oculomotor innervates the levator palpebrae superioris, which elevates the upper eyelid, and the oculomotor nerve also provides parasympathetic innervation to the smooth muscle of the interior of the eyeball: the constrictor muscle of the pupil; and the ciliary muscle, which changes lens curvature in the process of accommodation, the bringing of light rays to a focus on the retina. In the domestic mammals, the striated muscles that move the eyeball are the four rectus muscles, medial, lateral, dorsal and ventral; the dorsal and ventral oblique muscles, and the retractor bulbi muscle. Of these muscles, all but the dorsal oblique, lateral rectus and retractor bulbi are innervated by the oculomotor nerve. The dorsal oblique is innervated by the trochlear nerve. The lateral rectus and retractor bulbi are innervated by the abducent nerve (that is, according to some workers; several European texts state that only the lateral part of the retractor is supplied by the abducent, the remaining medial portion by the oculomotor). With respect to the retractor, it arises always directly medial to the lateral rectus. This is not determinative of the question but lends some support to the idea that the retractor is split off the lateral rectus and that both muscles receive their motor innervation from the abducent nerve alone. The eyeball and its attaching extraocular muscles are conical in form and are enclosed within the periorbital membrane, which extends from the margin of the orbit to the perimeter of the optic canal and orbital fissure. Medially the periorbital membrane is fused with the periosteum of the bony orbital wall. Within the periorbita, the eyeball rests on a fat pad and is freely movable, its movements determined by the balance of impulses to opposing muscles: Dorsal and ventral rectus muscles, which turn the eyeball so that the gaze is upward or downward, respectively; medial and lateral rectus muscles, which turn the eyeball’s gaze medially and laterally, respectively; and impulses to the oblique muscles, which are not strictly, but nearly, antagonistic. All of these muscles, except the ventral oblique, take origin internal to the periorbita from the perimeter of bone at the margin of the optic canal and orbital fissure (the orbital fissure is incorporated in the foramen orbitorotundum in swine and cattle) and insert in the fibrous sclera of the eyeball. The rectus muscles are the largest and strongest muscles attaching to the eyeball and each inserts by a thin, flat tendon anterior to the eyeball’s equator. The retractor bulbi, which is not present in humans, some other primates, and birds, arises medial to the lateral rectus at the lateral margin of the orbital fissure and divides into four fascicles, which insert posterior to the equator; in the dog, at dorsomedial, dorsolateral, ventromedial, and ventrolateral positions. The retractor is deep to the rectus muscles. It is an expanded, thin muscle that envelops the eyeball and optic nerve posteriorly and draws the eyeball toward the muscle’s origin at the orbital fissure. This increases pressure within the space enclosed by the periorbital membrane and pushes out the third eyelid, which is loosely attached. When extruded, the third eyelid covers the ventromedial exposed aspect of the eyeball. The phenomenon has significance in tetanus infection in the horse in which the retractor is hyperactive and the third eyelid flashes each time that the muscle contracts. Fig. 1. Extraocular muscles of the horse, lateral view of the orbit with periorbital membrane largely cut away. The appearance is similar in all the domestic mammals. Figure is from Topographische Anatomie des Pferdes, W. Ellenberger u. H. Baum: 1896, Verlag Paul Parey lacrimal gland ventral oblique m. dorsal rectus m. lateral rectus m. ventral rectus m. periorbital membrane, partly removed and reflected medial rectus m. Fig. 2. Deep dissection of the extraocular muscles of the horse, lateral view of the orbit with lacrimal gland removed and periorbital membrane largely cut away. The appearance is similar (but not the same) in all the domestic mammals. Figure is from Topographische Anatomie des Pferdes, W. Ellenberger u. H. Baum: 1896, Verlag Paul Parey. The artist has moved the dorsal oblique a little dorsally to show the muscle more fully than it would normally be exposed in a strict lateral view. dorsal rectus m. (cut) ventral oblique m. trochlea dorsal oblique m. lateral rectus m. retractor bulbi m. lbimm ventral rectus m. The dorsal oblique arises at the medial margin of the optic canal. It is smaller and weaker than the rectus muscles, spindle-shaped, and lies internal to the periorbita against the dorsomedial orbital wall. It is directed rostrodorsally toward the orbital margin and a depression of the medial wall that is bridged by the trochlear cartilage. The muscle tapers as it passes between the medial wall and the cartilage and, emerging between the two, turns posterolaterally to its attachment dorsally on the sclera; at its attachment, the tendon is posterior to the equator of the eyeball and lateral to the optic axis. The tendon is deep to the dorsal rectus muscle. Contraction of the muscle turns the dorsal aspect of the eyeball forward and medially. Since the attachment is to a spherical eyeball, the gaze is directed ventrolaterally. The ventral oblique arises from the medial wall of the orbit; in the dog, on the fibrous membrane that covers a small regularly appearing separation of the palatomaxillary suture at the medial wall of the maxillary foramen. The muscle passes laterally, ventral to the ventral rectus, and inserts posterior to the equator and lateral to the optic axis. The tendon inserts deep to the lateral rectus muscle on the lateral aspect of the eyeball. Its contraction rotates the eyeball, turning its dorsal aspect laterally and the gaze a little upward (dorsally). Eye movement due to the oblique muscles is not easily detected on observing the animal as the movement is slight and is incorporated in the total movement of the eyeball. Paralysis of the dorsal oblique muscle is rare. It results in an unopposed contraction of the ventral oblique with an exaggerated upward gaze of the affected eye. With oculomotor nerve (ventral oblique; medial, dorsal and ventral rectus) paralysis, lateral strabismus is the predominant sign. Fig. 3A, Dorsal view, attachment of the dorsal oblique in humans; Fig. 3B, lateral view, attachment of the ventral oblique in humans. To the writer’s knowledge, no detailed work comparable to the work providing these figures has been done on the anatomy of our domestic animals. Figures are from http://www.cybersight.org/data/1/rec_docs/87_Ch%203%20%20Summary%20of%20the %20Gross%20Anatomy%20of%20the%20Extraocular%20M uscles,%20p.%2038-51.pdf. Fig. 3A Fig. 3B dorsal (super.) oblique tendon Fig. 4. Skull, canine. Lateral view with zygomatic arch removed. The depression bridged by the trochlea of the dorsal oblique and the origin of the ventral oblique are marked. depression bridged by trochlea gap in the palatomaxillary suture, in life, covered by membrane from which the ventral oblique takes origin Contraction of the rectus and oblique muscles is utilized to effect the delicate movements that keep the area of visual interest centered on the macular area of the retina. The innervation of these muscles and their action on the eyeball become significant chiefly in cases of paralysis but will be a consideration in the case of a muscle’s not functioning for any reason. Thus, with paralysis of the abducent nerve, the gaze on the affected side remains always medial, and so on. Movements of the eyeball are coordinated to maintain the area of visual interest focused on the macular area, or the area of the retina providing most acute vision, which varies in form according to species. These movements are often quite precise and the motor unit of each motor nerve fiber will be small. Different from the innervation of muscles that effect coarse movements, e.g., the bicep femoris, the triceps brachii, in which a single nerve fiber may innervate more than one thousand myofibers, a single nerve fiber of cranial nerves III, IV, and VI innervates perhaps only 10 myofibers. Moreover, the eye muscles provide a rich source of neuromuscular spindles, which furnish the necessary feedback of muscle length that enables precision in coordinate contraction and relaxation of muscle fibers. The proprioceptive fibers that innervate the extraocular muscles are all from the trigeminal. Thus, in addition to its motor innervation, every extraocular muscle receives as well trigeminal fibers, which mediate proprioception (Proprioceptive knowledge of eye position, Steinbach, M.J., Vision Research, 27, 1737 – 1744, 1987) and, probably, pain. These sensory fibers probably reach cranial nerves III, IV, and VI, as those nerves pass in proximity to the ophthalmic nerve in relation to the cavernous sinus or through the orbital fissure. Oculomotor Nerve. The oculomotor nerve passes from the ventromedial aspect of the crus cerebri, perforates the arachnoidea and the dura mater of the floor of the cranial vault and enters the orbital fissure, accompanied by the trochlear, abducent, and ophthalmic nerves, and the emissary vein of the orbital fissure, which joins the cavernous venous sinus to the orbital plexus of veins (dog, cat, Equidae; in ruminants and swine, the homologous vein is designated the emissary vein of the foramen orbitorotundum). As it emerges from the medial part of the orbital fissure, the oculomotor nerve divides into a dorsal branch, which supplies the dorsal rectus and levator of the upper eyelid, and the medial rectus and a ventral branch which supplies the ventral rectus and the ventral oblique, and bears the parasympathetic fibers which form the parasympathetic root of the ciliary ganglion. The arrangement of these branches, excepting the parasympathetic root of the ciliary ganglion, is shown in yellow in Fig. 5. The position of the ciliary ganglion is shown in Fig. 5. The parasympathetic nucleus of the oculomotor nerve occupies the ventrolateral periaqueductal gray of the midbrain just dorsal to the oculomotor nucleus. Its position, as it appears in the red kangaroo, can be seen in Fig. 6. The smaller animals are closer to the ground and have a greater use of the muscle of accomodation for focussing on near-objects. The smooth muscle of accomodation is better developed in the dog and cat than in the horse and a greater number of ganglion cells that supply the muscle is reasonably expected. Ellenberger-Baum (1943) states that the ganglion is absolutely largest in the cat. Parasympathetic ganglia generally receive three kinds of fibers: 1. Preganglionic parasympathetic fibers, the “parasympathetic root”; 2. Sensory fibers, the sensory “root”; and 3. Sympathetic fibers make up the sympathetic “root”. Parasympathetic fibers synapse in the ganglion; sensory and sympathetic fibers pass through the ganglion without synapse. The ciliary ganglion’s parasympathetic root passes from the ventral branch of the oculomotor; its sensory root, from the long ciliary nerve, a branch of the nasociliary branch of the opththalmic, and the sympathetic root is thought to proceed from the nerve of the pterygoid canal. The nerves that pass from the ganglion--- in the case of the ciliary ganglion, the short ciliary nerves--- are a common path for the three kinds of fibers. The short ciliary nerves perforate the sclera in a circular arrangement around the optic nerve and enter the choroidea. Sympathetic fibers supply the dilatator of the pupil; parasympathetic fibers supply the constrictor muscle of the pupil and the muscle of accomodation; sensory fibers form neuroreceptor synapses with receptors for pain, touch and pressure. Reflexes mediated by the autonomic (sympathetic, parasympathetic) fibers of the ciliary nerves: 1. determine the size of the pupil in response to light and darkness; 2. provide the narrowing of the pupil associated with accomodation; 3. provide the changes in the curvature of the lens in the process of accomodation. The sensory fibers of the ciliary nerves mediate the oculocardiac reflex in which increasing pressure within the eyeball results in a slowing of the heart rate. In the text Human Physiology (Bernardo Houssay et al.: 1955, McGraw Hill) is recited the physiological correspondence of intraocular pressure and blood pressure. The oculocardiac reflex appears to be general; that is, placing digital pressure on the eyeball of an animal results in a slowing of the heart rate. Fig. 5. Canine, anterior view of structures at the apex of the orbit. m. levator palpebrae superioris m. rectus dorsalis m. retractor bulbi oculomotor n., dorsal branch ventral branch branch to m. obliquus ventralis m. obliquus dorsalis m. rectus lateralis optic n. m. rectus medialis position of ciliary ganglion m. rectus ventralis Fig. 6. Myelin-stained section at the level of the rostral midbrain of the red kangaroo (from: Brain Biodiversity Bank, Michigan State University: www.msu.edu/~brains/brains/redkangaroo/sections/redroo_sec1103.jpg). parasympathetic nucleus of the oculomotor nerve oculomotor nucleus red nucleus oculomotor nerve fibers; they pass through the medial part of the red nucleus and emerge from the midbrain medial to the crus cerebri crus cerebri Fig. 7. Canine brain, lateral view with left hemisphere removed. The origin of the oculomotor, trochlear, trigeminal, and abducent nerves is indicated. IV V crus cerebri III VI Fig. 8. Canine brain, dorsal view with hemispheres (in part) and cerebellum (entirely) removed. The origin of the trochlear and trigeminal nerves is indicated. IV V Fig. 9. Canine brain, ventral view. The olfactory bulb (designated I, here) and the origin of the optic, oculomotor, trochlear, trigeminal (V), and abducent nerves is indicated. I II III IV V VI Trochlear Nerve. The trochlear nerve arises from the midbrain at the level of the caudal (posterior) colliculus. The trochlear nucleus is ventral to the periaqueductal gray in a paramedian position at rostral (anterior) levels of the caudal colliculus. It is separated from the oculomotor nucleus by an interval of perhaps .5 cm in the dog. Fig. 10. Canine brain, sagittal section, myelin hematoxylin stain. From The Brain of the Dog in Section, Plate 60, Marcus Singer, 1962: Saunders. nuclei of the oculomotor and trochlear nerves in the ventrolateral periaqueductal gray Fibers pass caudally from the trochlear nucleus and enter the anterior (rostral) medullary velum of the fourth ventricle where they incline sharply medially, decussating with the contralateral fibers. Following decussation, the fibers emerge dorsally from the midbrain beneath the caudal colliculus and, within the subarachnoid space, pass laterally and turn rostroventrally alongside the midbrain. They perforate the dura of the tentorium cerebelli and continue rostrally with the third, fifth, and sixth cranial nerves in relation to the cavernous sinus. The third, fourth, and sixth cranial nerves and the ophthalmic branch of the fifth with the emissary vein of the orbital fissure continue rostrally through the orbital fissure, emerging at the apex of the orbit where the trochlear nerve enters the dorsal oblique muscle. Fig. 11. Sheep brain at the level of the decussation of the trochlear nerve in the rostral medullary velum. Myelin stain. The rostral end of the fourth ventricle can be seen ventral to the velum. trochlear nerve Fig. 12. Canine brain, median section. mesencephalic aqueduct rostral colliculus caudal colliculus decussation of trochlear nerve within the rostral medullary velum cerebellum Fig. 13. Equine orbit, deep dissection, lateral view. The dorsal rectus is removed in part to expose the dorsal oblique, which the artist has moved a little dorsally in what would otherwise be a strict lateral view. In this figure, the dorsal oblique is emphasized and the trochlear nerve is shown in yellow. Figure is from Topographische Anatomie des Pferdes, W. Ellenberger u. H. Baum: 1896, Verlag Paul Parey. medial rectus m. dorsal rectus m. (cut) trochlea frontal n. dorsal oblique m. infratrochlear n. trochlear n. ethmoidal n. fFig.14. Canine, rostral view of the nerves, vessels, and muscles at the level of the optic canal and orbital fissure. The optic canal transmits the optic nerve and internal ophthalmic artery (not shown in this figure); the orbital fissure transmits other vessels and nerves that supply the orbit: emissary vein of the orbital fissure, oculomotor, trochlear (not shown in this figure), abducent, and ophthalmic nerves. ophthalmic nerve: lacrimal, frontal, ethmoidal, nasociliary, long ciliary abducent nerve ethmoidal artery aaa emissary vein, orbital fissure optic n. oculomotor nerve nerve The trochlear nerve is not shown in Figs. 5 or 14 and I have not traced it. In humans, it passes medially from the orbital fissure caudal to the origin of the levator palpebrae and the dorsal rectus, then onto the dorsolateral aspect of the dorsal oblique and extends along the deep, lateral, aspect of the muscle, which it enters. Paralysis of the dorsal oblique leaves the ventral oblique unopposed and the gaze is directed dorsally. Fig. 15. Canine, left orbit, with much of the tissues removed to show the veins of the medial orbital plexus. Note that the ethmoidal a./v. pass medial to the dorsal oblique muscle; the ethmoidal n., lateral to the dorsal oblique, then between it and the medial rectus to enter the more ventral of the two ethmoidal foramina. venous trunk joining angular vein of the eye and the emissary vein of the orbital fissure dorsal oblique m. ethmoidal a./v. angular vein of the eye ethmoidal n. medial rectus m. emissary vein of the orbital fissure optic nerve emissary vein of the round foramen (enters the rostral alar foramen) deep facial vein ethmoidal foramina optic canal orbital fissure rostral alar foramen Abducent Nerve. The nucleus of the abducent nerve is located at the pontomedullary junction a little below the floor of the fourth ventricle. The nucleus is ventrolateral to the genu of the facial nerve and lateral to the medial longitudinal fasciculus. Its fibers, all of them motor, pass ventrally, emerging at the caudolateral angle of junction of the pyramid and trapezoid body. From this point the nerve passes forward in the subarachnoid space and perforates the dura, joining the 3rd, 4th and 5th cranial nerves in relation to the cavernous sinus. With the ophthalmic branch of the trigeminal and the emissary vein, all depart the cranial cavity at the orbital fissure and enter the apical part of the orbit. The abducent nerve is most lateral as it emerges from the fissure and gives off branches to the retractor bulbi and the deep, medial, surface of the lateral rectus. Fig. 16. Canine brain, cross-section at pontomedullary junction, hematoxylin stain. From The Brain of the Dog in Section, Marcus Singer, 1962: Saunders. Inset is taken from the main figure and labeled particularly for the abducent nucleus. genu, facial nerve medial longitudinal fasciculus abducent nucleus abducent nerve fibers Fig. 16. Canine brain, lateral view with left hemisphere removed. Trapezoid body, pyramid, and abducent nerve are marked. trapezoid body abducent nerve pyramid Fig. 17. Relations at the orbital fissure. position of orbital fissure (dashed line) ophthalmic nerve branches abducent n. oculomotor n. lateral rectus and retractor bulbi emissary v. of the orbital fissure Summary: The 3rd, 4th, and 6th cranial nerves innervate the striated muscles that are responsible for movements of the eyeball. The 3rd cranial nerve also innervates the striated proper levator of the upper eyelid and the pupillary constrictor and ciliary smooth muscle. 1. When a nerve supplying any striated (skeletal) muscle is injured, myofibers affected will cease to function at once and these myofibers will begin to atrophy. In the case of nerves supplying smooth muscle, in general, only its regulation is lost. In the case of the pupillary constrictor, it loses its regulation but the pupillary dilator is still receiving innervation and is functional. The result is a dilated pupil that does not constrict in response to light. Loss of ciliary smooth muscle innervation with failure of accommodation is not generally detected in our animals; loss of accomodation would be a source of complaint by persons, who would find be unable to focus on near-objects on the affected side. 2. Injury to the oculomotor nerve peripherally, depending on location of the injury and the degree of involvement, is most obvious as a lateral strabismus (the affected eye directed laterally), mild drooping of the upper eyelid, and a dilated pupil on the affected side. If the injury is central, depending on the size and location of the injury, a number of additional signs could be present. In this regard, it should be noted that most or all of the fibers supplying the dorsal rectus come from the contralateral oculomotor nucleus. This would be of no consequence in the case of a peripheral oculomotor lesion but, with a central lesion, would affect oculomotor eye muscles of the affected side save for the dorsal rectus which would be paralyzed on the opposite side. 3. Peripheral injury to the trochlear nerve with loss of dorsal oblique function results in an unopposed ventral oblique and an upward deviated eye. If the injury is central, depending on the location and extent of the injury, a number of additional signs could be present. 4. Peripheral injury to the abducent nerve results in a medial strabismus and inability to retract the eyeball. Again, as with the oculomotor and trochlear nerves, if the injury is central, a number of additional signs could be present. This concludes this presentation.