JACC: Heart Failure
advertisement

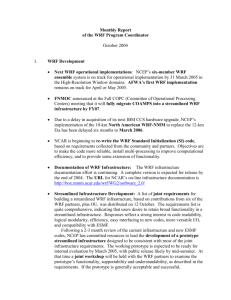
Supplementary Data Methods: Statistical Analysis of Risk Score In a stepwise backward Cox regression analysis was carried out with all univariately associated variables. After this model was constructed, optimal cut off points were determined by the highest sum of specificity and sensitivity calculated using receiver operator curve analysis. Cut offs for the model were then chosen at clinical relevant or numerical easy cut off points. In sensitivity analysis, bootstrapped forward Cox regression was carried out via the swboot syntax in STATA to investigate the relative importance of each included variable. Internal validation of additive power of KIM-1 to the model was carried out by comparison of Harrell’s C indices in two randomly created datasets from the entire study population by using the Somersd syntax in STATA. With the dichotomized variables a new model was constructed, and based on this model a risk score was created based on the individual X2 values of each variable in the multivariable model. For simplicity, this model did not include interaction terms. Finally, quartiles of this risk score were investigated for the relationship with WRF. Results: Risk score for WRF On the basis of the final stepwise Cox regression model, we determined optimal cut-off values for each variable in the model. Table 3 shows the cut-off values and the multivariable HR for each variable after dichotomization. Afterwards, we constructed a risk model for WRF with weights of each variable based on Chi2 values as presented in the last column of Supplementary Table 3. The maximum score of this risk score is 54 points, which was present in 1 patient, while in 51 patients the minimum score of 0 was present. Mean risk score was 20 ± 11 points. Among quartiles of the risk score, the risk for WRF increased with higher quartiles of the risk score. However, quartile 2 and 3 did not differ in their risk for WRF. Therefore, for better risk stratification, taking these groups together resulted in three groups (Supplementary Table 4). In these three groups a risk score 13 – 28 was associated with increased risk for WRF HR 2.63, 95% CI 1.77 to 3.89, P < 0.001, while a risk score > 28 carried the highest risk: HR 6.08, 95% CI 4.09 to 9.04, P < 0.001 (both versus risk < 13) (Supplementary Figure 1). Alternatively, since the middle groups is a representation of the mean study population, the relative risk in relation to a risk score of 13 – 28 for a risk score < 13 was HR 0.38, 95% CI 0.26 to 0.56, P < 0.001, and for a risk score > 28 HR 2.32, 95% CI 1.80 to 2.96, P < 0.001. Using the alternative definition of an absolute increase in serum creatinine (> 0.3mg/dL), we found very similar results. A risk score 13 – 28 showed a HR 2.63, 95% CI 1.77 to 3.89, P < 0.001, while a risk score > 28 carried also using this definition the highest risk for WRF: HR 7.56, 95% CI 5.21 to 11.0, P < 0.001. Bootstrapped Harrell’s C for this model with this definition of WRF was 0.703 (0.675 – 0.731), P < 0.001. Supplementary Table 1. Variable selection on the basis of bootstrapped stepwise Cox regression Number of replications out of 100 in which factor selected Variable Model without With KIM-1 With NAG With NGAL tubular markers KIM-1 NA 85 NA NA NAG NA NA 4 NA NGAL NA NA NA 25 eGFR 79 72 81 79 UACR 89 30 85 79 BMI 58 44 45 56 LVEF 52 44 41 50 COPD 37 42 56 38 Furosemide use 38 34 33 39 ASA use 33 47 27 25 Hemoglobin 30 25 28 29 Age 46 21 34 39 Diabetes 20 21 13 16 Digoxin use 16 10 16 11 Creatinine 13 20 13 13 DBP 6 6 7 5 Nitrate use 11 14 6 11 CVP>6 cm H2O 5 15 13 8 Beta-blocker use 9 10 12 6 Amiodarone use 12 10 8 16 NYHA class III/IV 10 11 8 14 Spironolactone use 11 2 9 9 Heart Rate 7 5 5 5 Atrial Fibrillation 2 2 2 2 Gender 0 1 1 1 P value for entering and remaining in the model 0.01 and 0.02. Abbreviations as in Table 1. Supplementary Table 2: Reclassification Model with KIM-1 Model without KIM-1 Risk Reclassification 0% to < 5% 5% to < 10% 10% to <20% > 20% Total Higher Lower Persons Included 54 2 0 0 56 No. of events 1 0 0 0 1 0 NA No of nonevents 53 2 0 0 55 2 NA Persons Included 56 452 100 0 608 No. of events 0 33 16 0 49 16 0 No of nonevents 56 419 84 0 559 84 56 Persons Included 0 153 656 161 879 No. of events 0 17 100 36 150 36 17 No of nonevents 0 136 556 125 817 125 136 0% to < 5% 5% to < 10% 10% to < 20% > 20% Persons Included 0 0 97 280 377 No. of events 0 0 10 77 87 NA 10 No of nonevents 0 0 87 203 290 NA 87 110 605 853 441 2011 1 50 126 113 290 52 27 109 555 727 318 1721 209 279 Total Persons Included No. of events No of nonevents Abbreviations: KIM-1: Kidney Injury Molecule 1 Supplementary Table 3. Risk Score for WRF and cut off points Variable Multivariable HR p-Value X2 Score Factor KIM (> 3500 ng/gCr) 1.87 (1.47 to 2.38) < 0.001 25 15 1.7 eGFR (< 60 mL/min/1.73m2) 1.64 (1.28 to 2.09) < 0.001 16 9 1.8 LVEF (< 30%) 1.45 (1.14 to 1.85) 0.002 9 6 1.5 COPD (yes) 1.50 (1.15 to 1.95) 0.003 9 6 1.5 Hb (< 14 g/dL) 1.46 (1.13 to 1.88) 0.004 8 5 1.6 Loop Diuretics (yes) 1.53 (1.11 to 2.09) 0.009 7 4 1.8 BMI (> 28 kg/m2) 1.34 (1.05 to 1.72) 0.021 5 3 1.7 Aspirin use (no) 1.31 (1.03 to 1.67) 0.027 5 3 1.7 Age (>75 years) 1.36 (1.04 to 1.77) 0.024 5 3 1.7 Total Score 54 Abbreviations as in Table 1. Factor is ratio between X2 and Score. Bootstrapped Harrell’s C with 100 replications: 0.677 (0.646 to 0.708), p < 0.001) (total dataset). The risk score is calculated based on the presence or absence of the variable specified in the first column. If present, the number in the corresponding 4th column is added to the score. Supplementary Table 4. Risk score for WRF Variable N Hazard Ratio (95% CI) P-Value Risk Score 0 – 12 577 1.00 (ref) - Risk Score 13 – 19 473 2.64 (1.71 to 4.05) < 0.001 Risk Score 20 – 28 512 2.61 (1.71 to 4.01) < 0.001 Risk Score 29 – 54 449 6.08 (4.09 to 9.04) < 0.001 Risk Score < 13 577 1.00 (ref) - Risk Score 13 – 28 985 2.63 (1.77 to 3.89) < 0.001 Risk Score > 28 449 6.08 (4.09 to 9.04) < 0.001 Risk Score < 13 577 0.38 (0.26 to 0.56) < 0.001 Risk Score 13 – 28 985 1.00 (ref) - Risk Score > 28 449 2.32 (1.80 to 2.96) < 0.001 These risk groups represent groups of patients with similar risk scores. These scores have been calculated based on the calculation of the risk score in supplementary table 3. Supplementary Figure 1. Risk Score and WRF