Working Draft ITP Program Model 2014-1
advertisement

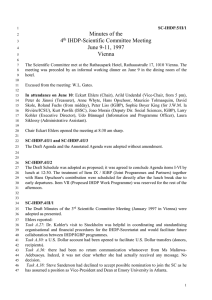
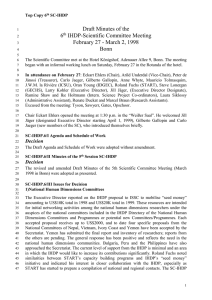
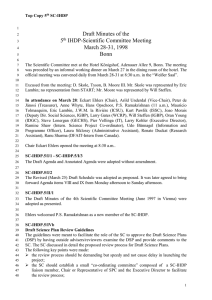
Working Draft Guiding Principles of the Howard County Infants and Toddlers Program The participants of the Howard County Infants and Toddlers Program believe in family-centered practices to address each child’s needs in natural environments. The following seven principals outlined by the OSEP Workgroup on Principles and Practices in Natural Environments (February, 2008) guide our practice. 1 Infants and toddlers learn best through everyday experiences and interactions with familiar people in familiar contexts. 2 All families, with the necessary supports and resources, can enhance their children’s learning and development. 3 The primary role of the service provider in early intervention is to work with and support the family members and caregivers in a child’s life. 4 The early intervention process, from initial contacts through transition, is dynamic and individualized to reflect the child’s and family members’ preferences, learning styles and cultural beliefs. 5 IFSP outcomes are functional and based on children’s and families’ needs and priorities. 6 The family’s priorities, needs and interests are addressed most appropriately by a primary provider who represents and receives team and community support. 7 Interventions with young children and family members are based on explicit principles, validated practices, best available research and relevant laws and regulations. Working Draft Implementation Team Collaborative, multidimensional assessment to determine eligibility and identify strengths and needs Linda Flanagan, Instructional Facilitator, Countywide Services Jen Harwood, Project Facilitator, Early Intervention Services Anne Hickey, Instructional Facilitator, Early Intervention Services Jane Jung-Potter, Program Head, Physical Therapy Collaborative consultation to child care to enhance the staff's capacity to help the child between visits Emily Kinsler, Instructional Facilitator, speech and Language Pathology Joan Ogaitis, Program Head, Occupational Therapy Stephanie Wickstrom, Early Intervention Specialist/Cluster Lead Vacancy Vacancy Support-based home visiting to build the capacity of each familiy to enhance learning between visits Family assessment to help families set priorities and outcomes HCITP Program Model to Support Achievement of Child and Family Outcomes Functional, participation-based child and family outcomes Vacancy Integrated services through a flexible, primary service provider model Working Draft Component Policy Evidence-base Alignment with HCPSS Strategic Plan Family assessment to help families set priorities and outcomes Family assessment and multidimensional assessment as defined in COMAR 13a.13.01.05, …ongoing multidisciplinary assessment of the child and the familydirected assessment of the resources, priorities and concerns of the family, as it relates to the needs of the child in the development of integrated outcomes for the IFSP . IDEA CFR 303.321(a)(2), A statement of the family’s concerns, priorities, and resources related to enhancing the development of the child as identified through assessment, with the concurrence of the family. As defined in COMAR 13A.13.01.08 and IDEA CFR §303.344. A statement of the measurable results or outcomes considered developmentally appropriate and expected to be achieved for the child and family. As defined in COMAR 13A.13.01.08, Services based on peer-reviewed research that are necessary to meet the unique needs of the child and the family to achieve the results or outcomes. As specified in IDEA CFR §303.12(b)(3) Providers are responsible for consulting with and training parents and others concerning the provision of early intervention services described in the IFSP of the infant or toddler with a disability. Additionally, this consultation and training will provide family members and others with the tools to facilitate a child’s development even when a teacher or therapist is not present. Guidance from Professional Organizations (CEC/DEC, NAEYC, ECTA, MSDE) • Agreed-Upon Mission and Key Principles for Providing Early Intervention Services in Natural Environments • Seven Key Principles: Looks Like Doesn’t Look Like • Agreed-Upon Key Practices in the Early Intervention Journey • Occupational and Physical Therapy Early Intervention and School-Based Services in Maryland http://ectacenter.org/ & HCPSS site Selected Research “Family involvement results in significantly greater intervention effects “(Shonkoff & Hauser-Cram, 1987; Ketelaar, Vermeer, Helders, & Hart, 1998) STUDENT ENGAGEMENT Outcome 1.4: Students are engaged in the learning process. 1.4.4 Provide authentic learning experiences to solve real-world problems. STUDENT WELL-BEING Outcome 1.7: Schools support the social and emotional safety and well-being of all students. 1.7.5 Ensure students have access to culturally proficient professional staff members who support them and help them solve problems. STAFF PERFORMANCE Outcome 2.3: Staff members are held accountable for and supported in meeting performance expectations. 2.3.2 Provide a professional learning program that supports all employees in meeting performance expectations. FAMIIES AND COMMUNITY COLLABORATION AND WELLBEING Outcome 3.1: HCPSS collaborates with family and community partners to engender a culture of trust, transparency, and mutual respect. 3.1.5 Develop intentional strategies to involve parents in decisions regarding their child’s HCPSS experience. 3.1.6 Develop intentional strategies to connect directly with families who need additional supports Outcome 3.4: HCPSS supports the well-being of students and families. ORGANIZATION PERFORMANCE Outcome 4.6: Decisions are informed by relevant data in all operational areas. 4.6.1 Regularly consider research-based best practices. 4.6.2 Consistently include collaborative stakeholder teams in planning processes to inform decisions. 4.6.4 Develop evaluation plans for all pilots and refine programs based on evaluation results. Collaborative, multidimensional assessment to determine eligibility and identify strengths and needs Functional, participation-based child and family outcomes Integrated services through a flexible, primary service provider model Support-based home visiting to build the capacity of each family to enhance learning between visits Collaborative consultation to child care to enhance the staff's capacity to help the child between visits “Programs focused on family strategy use were more effective than other family participation methods”(Shonkoff & Hauser-Cram, 1987) “Intervention effects dependent upon supporting families in using effective interaction strategies” (Mahoney, Boyce, Fewell, Spiker, Wheeden, 1998) See attachment, The Importance of Family Strategy Use to Promote Child Development See attachment: Selected Bibliography Working Draft Component Family assessment to help families set priorities and outcomes Collaborative, multidimensional assessment to determine eligibility and identify strengths and needs Procedure/Practice All families will participate in a RoutinesBased Interview, including ecomap, completed as part of evaluation and assessment process. (or document denial of consent) All service providers will embed ongoing assessment of concerns, priorities and resources into practice. All service providers will complete collaborative evaluations and assessments using DAYC-2 and other approved tools. All service providers will ensure family participation in COS entrance and exit ratings. Functional, participation-based child and family outcomes Each outcome is understandable, observable, functional, and linked to a family concern. Integrated services through a flexible, primary service provider model 90% of eligible children and families will receive a weekly home visit by a primary service provider. Co-visits as needed to support the primary service provider. 100% of service providers will implement support-based home or community visiting practices. Support-based home visiting to build the capacity of each family to enhance learning between visits Collaborative consultation to child care to enhance the staff's capacity to help the child between visits Timeline/Fidelity Measure/Target By September 1, 2014 100% of returning service providers will complete a RBI training with 90% accuracy as measured by the implementation checklist. (new service providers will begin process with completion by January, 2015 or subsequent years.) Sept-June 2014 and beyond – annual rechecks completed with maintained accuracy for each provider. By January,2016 Howard County will meet or exceed the state target for Child Outcome Summary Indicator 3. % who entered below age expectations and increased their rate of growth by time of exit 7/1/15-12/31/15 Social Emotional Knowledge and Skills Adaptive Behavior 81.1% 86.3% 87.5% 1/1/15-6/30/15 target 70.36% 74.1% 78.56% 7/1/14-12/31/14 target 59.61% 61.63% 69.62% 1/1/14-6/30/14 pending pending pending pending 7/1/13-12/31/13 pending pending pending pending 1/1/13-6/30/13 actual 48.86% (81.1%) 48.89% (86.3%) 60.68% (87.5%) (state target) By June 30, 2014, 100% teams will conduct peer review using the Recommended Practice: Functional Outcomes Checklist. (Implementation team facilitation provided.) By December 1, 2014, the implementation team will review 4 outcomes from at least 2 children/families from each service provider. The FOC will indicate average rating of 3-4. By January,2015 data will indicate that 70% of eligible children and families are receiving a weekly home visit provided by a primary service provider. By September,2015, data will indicate the 90% of eligible children and families are receiving a weekly home visit provided by a primary service provider. September 1, 2014-January 31, 2015 100% of service providers will have the Support-Based Home Visiting Checklist completed and reviewed by the Implementation team. February 1, 2015-September 1, 2015 100% of service providers will receive an average rating of 3-4 on the Support-Based Home Visiting Checklist. September 1, 2015 and beyond – Each service provider will maintain an average rating of 3-4 on the SupportBased Home Visiting Checklist completed by the implementation team or peer review. Working Draft The Importance of Family Strategy Use to Promote Child Development • Families are considered the “engine of change” (Brooks-Gunn, Berlin, & Fuligini, 2000, p. 562) • Bronfenbrenner (1999) contends that family use of intervention strategies must be considered both an outcome of intervention and a level of intervention intensity • “...those adults who are most consistently available and committed to the child’s well-being play a special role in promoting competence and adaptation that cannot be replaced by individuals who are present less consistently or whose emotional commitment is not unconditional” (National Research Council, 2000, p. 389) • “...the time has come to stop talking about parent involvement and to commit to learning how such involvement can be accomplished across a range of family constellations, circumstances, and values” (Mahoney, Robinson, & Perales, 2004) Study Hart & Risley, 1999 Shonkoff & HauserCram, 1987 Ketelaar, Vermeer, Helders, & Hart, 1998 Mahoney, Boyce, Fewell, Spiker, & Wheeden, 1998 (Infant Health and Development Program, IHDP; Longitudinal Study of Early Intervention, LSEI; Play and Learning Strategies, PALS; Family- Centered Outcomes Study, FCOS) Sample 42 families interacting in everyday situations with 1- to 2- year olds (typically developing) Children enrolled in EI before 36 months Design Longitudinal study; monthly, hourlong observations Intervention None Meta-analysis of 31 selected EI studies Various studies Children with cerebral palsy and other motor disabilities • IHDP: 298 lowbirthweight premature infants • LSEI: 238 dyads in,EI (child mean age = 31 months • PALS: 21 teen motherinfant/toddler dyads • FCOS: 47 mother-child dyads Reviewed 10 studies that examined the impact of parental role in motor interventions Re-examined data of four independent intervention research studies: • IHDP: 3 IHDP sites, Randomized Control Trial • LEI: Multisite investigation; 6 sites with interaction data • PALS: pre-post with control group • FCOS: 12-month, fieldbased investigation Compared infant motor development when parental involvement was high and when low Various studies Torres & Buceta, 1998 24 infants (0-2 years) with Down syndrome Trivette, Dunst, & Hamby, 2010 910 families (children ranged from 1 to 89 months; 85% with or at risk for delays or disabilities) Meta-analysis SEM Child/Family Outcomes • More time parents talk to child, more rapid vocabulary growth and IQ at age 3 • Across family SES • “Extra, optional talk” a quality indicator • Parent involvement showed significantly greater effects than interventions without • Focus on parent strategy-use more effective than other ways parents participated Across studies: • Significantly better child outcomes with parent involvement and strategy use • IHDP: home, center, and parent group • LEI: various • PALs: 3-month; 24 sessions, 30 minutes each • FCOS: 36 community-based programs • Maternal responsiveness significant predictor of child development • E.g.,IHDP:Mother-childinteraction6times more of variance in child development than intervention group assignment • Intervention effects unlikely without quality parent interactions • Authors conclude that, when EI not only worked with parents but also helped them learn more effective ways of interacting with their children, general development was promoted Portage 3x per week for one hour; parents instructed how to use the program at home None • Motor development increased when parents highly involved • Motor development decreased when parent involvement low • HOME variable part of definition of “involvement” • Capacity-building help-giving and family systems intervention practices were significantly and directly related to parenting parent well-being • Parent well-being was significantly related to parent-child interaction and child development Working Draft Effective Practices in Early Intervention for Families and Their Infants and Toddlers, Bonnie Keilty, Ed.D. July 13, 2010 New York City LEICC Meeting Select Bibliography Bernheimer, L., & Weisner, T. (2007). “Let me just tell you what I do all day...”: The family story at the center of intervention research and practice. Infants and Young Children, 20, 192-201. Bruder, M.B. (2000). Family centered early intervention: Clarifying our values for the new millennium. Topics in Early Childhood Special Education, 20, 105-115. Bruder, M.B. (2001). Inclusion of infants and toddlers: Outcomes and ecology. In M.J. Guralnick (Ed.), Early childhood inclusion: Focus on change (pp. 203-229). Baltimore, MD: Brookes Publishing. Campbell, P. (2004). Participation-based services: Promoting children’s participation in natural settings. Young Exceptional Children, 8, 20-29. Cook Pletcher, L., & Younggren, N.O. (2013). The Early Intervention Workbook. Essential Practices for Quality Services. Baltimore, MD: Brookes Publishing. Crawford, M.J, & Weber, B. (2014). Early Intervention Every Day! Embedding Activities in Daily Routines for /young Children and Their Families. Baltimore, MD: Brookes Publishing. Dunlap, G., Ester, T., Langhans, S., & Fox, L. (2006). Functional communication training with toddlers in home environments. Journal of Early Intervention, 28, 81-96. Dunst, C., Bruder, M.B., Trivette, C., Raab, M., & McLean, M. (2001). Natural learning opportunities for infants, toddlers, and preschoolers. Young Exceptional Children, 4(3) 18-25. Dunst, C., & Dempsey, I. (2007). Family-professional partnerships and parenting competence, confidence, and enjoyment. International Journal of Disability, Development and Education, 54, 305318. Dunst, C., Hamby, D., Trivette, C., Raab, M., & Bruder, M. (2000). Everyday family and community life and children’s naturally occurring learning opportunities. Journal of Early Intervention, 23, 151164. Dunst, C., & Trivette, C. (1996). Empowerment, effective helpgiving practices and family-centered care. Pediatric Nursing, 22, 334-343. Guralnick, M. J. (1997). Second generation research in the field of early intervention. In M. J. Guralnick (Ed.), The effectiveness of early intervention (pp. 3-20). Baltimore, MD: Paul H. Brookes Publishing Co. Hanson, M.J, & Lynch, E.W. (2013) Understanding Families. Supportive Approaches to Diversity, Disability, and Risk. 2nd ed. Baltimore, MD: Paul H. Brookes Publishing Co Jung, L.A. (2003). More IS better: Maximizing natural learning opportunities. Young Exceptional Children, 6(3) 21-26. Jung, L. (2005). Can we all fit? Squeezing in better support with fewer people. Young Exceptional Children, 8(4) 19-27. Jung, L., & Grisham-Brown, J. (2006). Moving from assessment information to IFSPs: Guidelines for a family-centered process. Young Exceptional Children, 9(2) 2-11. Keilty, B. (2010). The Early Intervention Guidebook for Families and Professionals: Partnering for Success. New York: Teachers College Press. Keilty, B. (2008). Early intervention home visiting principles in practice: A reflective approach. Young Exceptional Children, 11(2) 29-40. Kim, J., & Mahoney, G. (2004). The effects of mother’s style of interaction on children’s engagement: Implications for using responsive interventions with parents. Topics in Early Childhood Special Education, 24, 31-38. McWilliam, R., & Scott, S. (2001). A support approach to early intervention: A three-part framework. Infants and Young Children, 13, 55-66. McWilliam, R. (2010). Routines Based Intervention: Supporting Young Children and Their Families. Baltimore, MD: Brookes Publishing Co. Maryland State Steering Committee for Occupational and Physical Therapy School-Based Programs. (2008). Occupational and Physical Therapy Early Intervention and School-Based Services in Maryland. A guide to practice. Rush, D.D, & Shelden, M.L. 2011). The Early Childhood Coaching Handbook. Baltimore, MD: Brookes Publishing Co. Shonkoff, J., & Hauser-Cram, P. (1987). Early intervention for disabled infants and their families: A qualitative analysis. Pediatrics, 80(5), 650-658. Trivette, C. (2003, June). Influence of caregiver responsiveness on the development of young children with or at risk for developmental disabilities. Bridges: Practice based research syntheses, 1(3). Asheville, NC: Research and Training Center on Early Childhood Development, Puckett Center. Wilson, L.L., Mott, D.W., Batman, D. (2004). The Asset-Based Context Matrix: A tool for assessing children’s learning opportunities and participation in natural environments. Topics in Early Special Education, 24, 110-120. Woods, J., & Kashinath, S. (2007). Expanding opportunities for social communication into daily routines. Early Childhood Services: An Interdisciplinary Journal of Effectiveness, 2, 137-154.