Application for Education Program in Canterbury, United Kingdom
advertisement

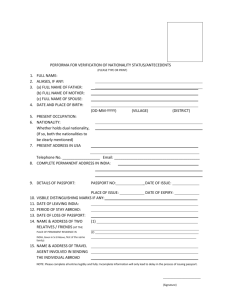
Information Sheet International Business Strategy and Culture Name (exactly as appears in official documents) E-mail Cell phone Home phone Address Birthdate (Month, date, year) Gender: M/F Academic Adviser Year in School U.S. Citizen Y/N Passport number (if available) Emergency contact name Cell phone E-mail Work phone Major Passport expiration Relationship to you Home phone Please answer the following questions in the space provided. Answers may be handwritten or typed. 1. Why do you want to participate in this MBA study tour? What do you hope to learn and experience through this visit to Brazil? . 2. Have you ever traveled abroad? If yes, when, where, why, and for how long? 3. How did you first learn about this program? Behavior code While abroad, I accept the responsibility of acting as a representative of both my country and Mount Mercy University. I will respect the laws of my host country, and maintain a high standard of conduct at all time. I understand that drug use, heavy drinking, or any behavior dangerous to myself or disruptive to the group will result in my expulsion from the program and my departure to the United States at my own expense. I will attend all classes, meetings, visits, and cultural excursions, and will be on time for group departures. If I miss a departure, I accept the responsibility to make my own way to the appointed place. I understand that I am not permitted to rent any cars, motorcycles or other power vehicles. Signed:_________________________________ Date:_____________________________________ Health Information Form Study abroad programs expose students to new environments and new activities. Long distance travel can create physical and mental stress that can trigger existing conditions. The information on this medical form will inform Mount Mercy staff of any pre-existing health conditions and help determine if consultation with your medical provider is recommended or required prior to travel. Failure to disclose relevant information can lead to a number of consequences, including difficulties with insurance, entry into a foreign country, and exclusion from the program. Health Information 1. Do you have any allergies? If so, what are the symptoms? How do you treat them? 2. Do you have any pre-existing health conditions? Have you been treated by a health care professional, other than for a routine check-up, at any point in the past five years? (This should include both physical and mental health conditions.) Please describe. 3. Are you taking any prescription medicine? If so, what? 4. Do you have any mobility issues or require any special accommodations? Travel abroad may involve climbing stairs, walking long distances, getting on and off public transportation. 5. Do you have any special dietary needs? (Vegetarian, diabetic, religious) Please describe. 6. Health insurance company 7. ID No 8. Group No 9. Name, address and phone number of personal physician Please attach a copy of your health insurance card. By signing this release, you acknowledge that the information is complete and authorize the sharing of this information with the program director and other Mount Mercy personnel as necessary and appropriate. Signature___________________________ Name (printed)_______________________ Date__________________________