Histo CH13 pp400-430 [12-10
advertisement

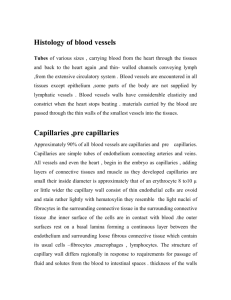
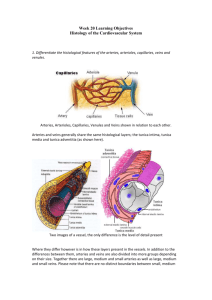
Histology Ch13, pp400-430 Cardiovascular System Overview of the Cardiovascular System o Cardiovascular system includes heart, blood vessels, and lymphatic vessels o Heart pumps arteries > arterioles > capillaries o In capillaries, 2-way fluid exchange occurs between blood and tissues Fluid (blood filtrate) carries O2 and metabolites through capillary walls In tissue, molecules exchanged for CO2 and waste products Most fluid reenters distal/venous end of capillaries, with remainder entering lymphatic capillaries Lymphatic vessels ultimately return this fluid to the blood stream o Arterioles, associated capillary network, and postcapillary venules form microcirculatory/microvascular bed o Veins collect blood from postcapillary venules and returns it to the heart o Two circulations distribute blood to body Systemic: blood from heart to tissues, and back Portal systems = vein or arteriole interposed between two capillary networks o Venous portal systems = Vessels carrying blood to liver (hepatic portal system) Vessels leading to pituitary (hypothalamic-hypophyseal portal system) Pulmonary: blood from heart to lungs, and back Heart o o o o o 2/3 on left side of thoracic cavity, in the middle mediastinum (enclosed by sternum, spine, diaphragm, and lungs) Surrounded by tough fibrous "pericardium" sac, which attaches heart to diaphragm and neighboring organs Heart maintains unidirectional flow of blood Valves (CT with overlying endocardium) prevent backflow of blood Fibrosa: Core of valve. Fibrous extensions from dense irregular CT of skeletal rings of heart. Spongiosa: Loose CT on atrial/blood vessel side of each valve. Acts as shock absorber. Ventricularis: Adjacent to ventricular surface. Covered in endothelium. Continues into chordae tendineae > papillary muscles. Valve heart disease causing degeneration (calcification, fibrosis) or inflammation (valvulitis) that leads to angiogenesis in normally avascular valve tissue > heart malfunction o Normally targets mitral (65-70%) or aortic (20-25%) valves Interatrial and interventricular septums separate R and L sides of heart Body > R atrium > R ventricle > Lungs Lungs > L atrium > L ventricle > Body Contains the following: Cardiac muscle: Contraction to propel blood Fibrous skeleton: 4 fibrous rings surrounding valve orifices (dense irregular CT), 2 fibrous trigones connecting the rings, and membranous part of interventricular/atrial septums (no muscle, dense CT, contains AV bundle). Attachment for atrial and ventricular myocardium + acts as electrical insultor. Conducting system: Initiation and propagation of rhythmic depolarizations. Purkinje fibers = modified cardiac muscle cells. Loss of rhythm > loss of circulation (cardiac arrest) > no Rx > sudden cardiac death Coronary vasculature: L/R coronary arteries + several cardiac veins (drain into coronary sinus) Walls composed of three layers: Epicardium: Visceral layer of serous pericardium adheres to outer surface of heart. Single layer of mesothelial cells and underlying CT/adipose tissue. Blood vessels and nerves here. Epicardium is reflected back at great vessels as parietal layer of serous pericardium. Cavity formed = pericardial cavity. Myocardium: Cardiac muscle. Principle component of heart. o o Endocardium: Inner layer of endothelium and subendothelial CT, middle CT/SM, and deeper layer of CT (subendocardial layer). Conducting system located in subendocardial layer. Intrinsic Regulation of Heart Rate Conducting system of the heart: SA and AV nodes Sinoatrial (SA) node: pacemarker of heart, located by SVC/right atrial junction (60-100bpm pace) Atrioventricular (AV) node: carries impulse into AV bundle (of His) (50bpm) Nodes are modified cardiac muscle that are smaller, contain fewer myofibrils, and lack intercalated discs AV bundle divides into L and R bundle branches >> subendothelial branches (aka Purkinje fibers) Fibers conduct impulse ~4x faster than cardiac muscle fibers Only elements to conduct impulse across fibrous skeleton Purkinje and bundle branches also modified muscle, but larger and do contain intercalated discs They are glycogen-rich >> more resistant to hypoxia than ventricular muscle cells Failure of the SA node > next fastest intrinsic rate will take over (usually AV node) "Complete heart block" > ventricles take over (30-40bpm) Systemic Regulation of Heart Rate Stimulation of parasympathetic (vagus - CN X) nerves decreases heart rate Acetylchoine causes bradycardia, reduces force, and constricts coronary arteries Stimulation of sympathetic nerves increases heart rate Norepinephrine causes tachycardia, increases force, and dilates coronary arteries Heart rate and force of contraction can be regulated by circulating hormones and other substances Positive inotropic and chronotropic actions: o Epinephrine (activate β-adrenergic receptors) and norepinephrine o Ca++, thyroid hormones, caffeine, theophylline, and cardiac glycoside digoxin Increase intracellular Ca++ levels in myocytes Negative inotropic and chronotropic actions: o Adrenergic-receptor antagonists (propranolol) or Ca++ channel blockers CNS monitors arterial pressure and heart function through specialized receptors within cardio system Baroreceptors: high-pressure receptors, sense arterial pressure in carotid sinus and aortic arch Volume receptors: low-pressure receptors, sense venous pressure in atria and ventricles Chemoreceptors: detect O2, CO2, and pH, located in carotid and aortic bodies General Features of Arteries and Veins o Layers of Vascular Wall (lumen to outside) Tunica Intima: 3 components Single layer of squamous endothelium Basal lamina (collagen, proteoglycan,s glycoproteins) Subendothelial layer (loose CT) Tunica Media: circumferrential arranged layers of SM Tunica Adventitia: collagenous + elastic fibers. Contains vessels and nerves in larger vessels. o Vascular Endothelium Functional properties change in response to stimuli (endothelial activation) Bacterial/viral antigens, cytotoxins, lipid products, complement products, hypoxia Activated cells exhibit new surface adhesion molecules and produce different cytokines, lymphokines, growth factors, vasoconstrictors/dilators, and blood coagulation molecules Endothelial cells participate in structural and integrity of the vascular wall Maintenance of selective permeability barrier Maintenance of nonthrombogenic barrier Modulation of blood flow and vascualr resistance Regulation and modulation of immune responses Hormonal synthesis and other metabolic activities Modification of the lipoproteins Endothelium controls contraction and relaxation of SM cells in tunica media > control local blood flow Endothelial-derived relaxing factor (EDRF) > relaxation of blood vessels Vasodilation effect attributed to action of NO Shear stress produced during interaction of blood flow with endothelial cells initiate relaxation via NO Vasodilation > decreased vascular resistance/blood pressure NO synthesized via endothelial nitric oxide synthase (eNOS) o Triggered by shear stress (dragging force of blood flow) o NO diffuses through cell into tunica media and binds guanylate cyclase in SM cytoplasm > increaes production of cGMP > activate SM protein kinase G (PKG) > negative effect on intracellular Ca++ >> SM relaxation Metabolic stress also contributes to SM relaxation via prostacyclin (PGI 2) o PGI relaxes SM and inhibits platelet aggregation o PGI binds SM > stimulates cAMP-activated protein kinase A (PKA) > phosphorylates myosin light chain kinase (MLCK) > prevents activation of Ca++-CaM complex o Relaxation WITHOUT change in intracellular Ca++ concentration Endothelium-derived hyperpolarizing factor (EDHF) o Acts on Ca++ dependent K+ channels > hyperpolarization > relax SM Endothelins produced by endothelial cells in physiologic and pathologic mechanisms of circulatory system Vasoconstriction increases vascular resistance and systemic blood pressure Endothelin family (ET1, ET2, ET3) > bind to their own receptors on epithelial cells/vascular SM Prostaglandin H2 > Thromboxane A2 > decrease rate of NO production or inactivate NO Arteries o Large Arteries (Elastic Arteries) - aorta, pulmonary artery, common carotid, subclavian, common iliac, brachioceph. Multiple sheets of elastic lamellae in their walls Pressure generated by L ventricle moves blood through arteries and stretches them Recoil during diastole serves to maintain arterial blood pressure and flow of blood Tunica intima consists of endothelium, subendothelial CT, and inconspicuous internal elastic membrane Endothelial cells contain Weibel-Palade bodies in the cytoplasm o Contain von Willebrand factor > important roles in platelet adhesion o P-selectin > neutrophil-endothelial cell recognition Endothelial cells participate in structural and functional integrity of vascular wall Produce vasoactive agents causing constriction/relaxation of vascular SM Tunica media consists of multiple layers of SM separated by elastic lamellae Thickest of the three layers in large arteries Fenestrations in elastic lamellae allow diffusion of substances within arterial wall Hypertension > number and thickness of lamellae increase No fibroblasts Tunica adventitia is relatively thin CT layer Prevents expansion of arterial wall beyond physiologic limits during systole Fibroblasts and microphages are principal cells Contains vasa vasorum (blood vessels) and nervi vascularis (nerves) o Medium Arteries (Muscular Arteries) - most of the "named" arteries More SM and less elastin in the tunica media than elastic arteries Tunica intima is thinner and contains prominent internal elastic membrane Tunica media composed almost entirely of SM (little elastic material, no fibroblasts) Tunica adventitia relatively thick and separated from media by external elastic membrane o Small Arteries and Arterioles Distinguished from one another by number of SM cell layers in tunica media Small arteries have up to 8 layers Arterioles have 1-2 layers Tunica adventitia is thin, ill-defined Arterioles control blood flow to capillary network by contraction of SM Slight thickening of SM at origin of capillary bed from an arteriole = "precapillary sphincter" Arterioles can dilate 60-100% and can constrict up to 40% Directs blood flow to where it's most needed Capillaries o Single layer of endothelium + basal lamina o Classification of Capillaries Continuous Capillaries Muscle, lung, and CNS Only allow passage of relatively small molecules Numerous pinocytotic vesicles Pericytes sometimes surround capillary. Contractile controlled via NO. Support + stability. Fenestrated Capillaries Endocrine glands and sites of fluid and metabolite absorption (gallbladder, kidney, GI) Provide channels across capillary wall Pinocytotic vesicles Discontinuous (Sinusoidal) Capillaries Liver, spleen, and bone marrow Larger in diameter and more irregular shaped Ex. Kupffer cells and Ito cells in liver o Functional Aspects of Capillaries Vasomotion (capillary blood flow) controlled through local and systemic signals Density of the capillary network determines total surface area available for blood/tissue exchange Related to metabolic activity of the tissue (more active > rich capillary network) Arteriovenous Shunts aka Arteriovenous Anastomoses o Allow blood to bypass capillaries by providing direct routes between arteries and veins o Commonly found in skin of fingertips, nose, and lips o Serve in thermoregulation of body surface o Constriction of SM (closing shunt) diverts blood through capillary bed Veins o o Venules and Small Veins Postcapillary Venules Endothelial lining + basal lamina and pericytes Endothelium is where vasoactive agents (histamien/serotonin) work Pericytes promote mutual proliferation and survival with vessels In lymph nodes = high endothelial venules (HEVs) Muscular Venules Unlike postcapillary venules, have of tunica media and thin adventitia Pericytes not found in muscular venules Small Veins: continuous with muscular venules Medium Veins - most of the named vessels (radial, tibial, popliteal veins) Valves are characteristic feature (DVT most common in lower limbs) Tunica intima, media (thinner than in arteries), and adventitia (thicker than media) o Large Veins - ex. superior/inferior vena cava and hepatic portal vein Tunica media is relatively thin, and tunica adventitia is relatively thick Tunica adventitia is muscular compared to medium veins Atypical Blood Vessels o Coronary arteries Medium-sized muscular arteries Originate from proximal ascending aorta and lie on surface of heart (epicardium) Walls are thicker than those of comparable arteries in upper/lower limb (extra SM in tunica media) Relatively loose tunica adventitia > allow continuous changes in vascular diameter o Dural venous sinuses Venous channels in the cranial cavity Broad space within the dura mater that are line with endothelium and devoid of SM o Great saphenous vein Long subcutaneous vein (foot > femoral vein) Unusual amount of smooth muscle in tunica media Numerous longitudinal SM bundles in intima and adventitia Frequently used for coronary artery bypass graft (CABG) o Central adrenomedullary vein Passes through adrenal medulla Irregularly arranged SM bundles in tunica media > irregularities in thickness of vascular wall Contraction enhances efflux of hormones from adrenal medulla into circulation Lymphatic Vessels o Unidirectional movement (via valves) of fluids from tissues to bloodstream o Lymphatic capillaries are more permeable than blood capillaries > collect excess protein-rich tissue fluid o Eventually converge into larger lymphatic vessels (ie, thoracic duct) that dump into large veins in base of neck o Before lymph returns to blood it passes through lymph nodes, where it's exposed to cells of immune system Clinical Correlation: Atherosclerosis o Complications >> ischemic heart disease, myocardial infarction, stroke, and gangrene of the limbs o Lesions develop in tunica intima of large elastic arteries following endothelial injury o Oxidation of LDL in tunica intima > monocytes enter tunica intima and differentiate into macrophages > phagocytize oxidized LDL >> foam cells >> form fatty streak >> fibrofatty plaque o Accumulation of lipid and loss of integrity of the endothelium > plaque progresses o In later development, blood stasis and clotting (thrombosis) may lead to occlusion of vessel Clinical Correlation: Hypertension o Sustained diastolic >90mmHg or systolic >140mmHg o Associated with atherosclerotic vascular disease and increased risk of cardiovascular disorder o Luminal diameter of small muscular arteries/arterioles is reduced > inc. vascular resistance o Vascular SM cells multiply > adds to thickness of tunica media o Some of the SM cells accumulate lipids > accelerated rate of lipid accumulation in vessel walls o Cardiac muscle affected by pressure overload > compensatory L ventricle hypertrophy (larger and less elastic) Clinical Correlation: Ischemic Heart Disease (aka ischemic cardiomyopathy) o Imbalance between supply and demand of O2 @ heart o Commonly caused by atherosclerosis (inc. with age, family history, hypertension, smoking, hypercholesterolemia, and diabetes) > lumina of coronary arteries progressively narrows via development of plaques o Blood flow becomes critical when it's reduced by >90% o Sudden occlusion of narrowed lumen by thrombus > acute ischemic event > angina pain >> infarction o Infarcted tissue will heal, but possibly with decreased contractility