Population Pharmacokinetics of Phenobarbital in Neonates
advertisement

Hoa Nguyen
Mo'tasem Alsmadi
Nathan Zimmerman
Charles Kramer
22S:138 Bayesian Statistics Fall 2010
Project Report
Development of Bayesian Hierarchical Model for Phenobarbital Neonatal
Population Pharmacokinetics
1. Introduction
From fetal life through adolescence, there are dramatic changes in pharmacokinetics and
pharmacodynamics due to the organ maturation and changes in body composition associated
with normal development. Accordingly, one of the major areas of the application of population
pharmacokinetics approaches is the analysis of drug concentration in pediatric population. To
overcome the frequent lack of dense data sets in pediatric clinical pharmacology because of
ethical and logistic constraints, clinical trial simulation techniques in Bayesian approach has
widely been applied.
Phenobarbital is an antiepileptic drug used in long-term treatment of seizures. It is widely
used for treatment of neonatal seizures, thus there have been several studies of phenobarbital in
pediatric pharmacokinetics published in literature. Because of sampling restrictions, it is often
difficult to perform traditional pharmacokinetic (PK) studies in neonates and infants2. Therefore,
the aim the present project was to determine kinetic parameters of phenobarbital after one or
more sustained doses of intravenous administration, using an iterative 3-stage Bayesian
algorithm for population pharmacokinetic approach.
2. Materials and methods
2.1.Data sources
Routine clinical data were collected on 59 pre-term infants given phenobarbital for
prevention of seizures during the first 16 days after birth3. Each individual received an initial
dose followed by one or more sustaining doses by intravenous administration. Dataset was
obtained with acknowledgement to the Resource Facility for Population Kinetics at
http://www.rfpk.washington.edu. It was displayed in Appendix I and contains subject identifier
(ID), time of concentration measurement (time, hr), dose amount (amt, mg/kg), and weight (kg),
vargar (apgar score), scores < 7 indicate some degree of asphyxia at birth, and plasma
concentration of phenobarbital (conc, mg/l).
2.2.Pharmacokinetics model
Data were treated by a one-compartment open pharmacokinetic model with first-order
elimination.
fe
Body
Concentration
IV bolus input
Drug in urine, feces..
Volume
1
𝐶𝑙
𝐶(𝑡) = 𝐶(0) × 𝑒 −𝑉𝑑×𝑡
𝑓𝑒 = 𝐶𝑙 × 𝐶(𝑡)
The fundamental pharmacokinetic structural parameters are total body clearance (Cl),
apparent volume of distribution (Vd). Samples of subjects in pediatric PK studies frequently
cover a wider relative range in body size than comparable studies in adults. Therefore, PK
parameters such as clearance and volume are usually functions of body size. To avoid the
covariate effect of body weight, note that in this data set, doses are specified (amt) in mg per
kilogram of body weight, thus, the disposition parameters Cl and Vd will automatically scaled by
body weight. Their units will be liters per hour per kilogram and liters per kilogram respectively.
In addition, no covariates such as apgar score, other body size were incorporated into this
population model. In order to get positive values from Bayesian estimates of parameters, the
subject specific vector of PK parameters was assumed to be drawn from a log-normal
distribution. In other word, 2 parameters of the model will be monitored by WinBugs, which are
log(Cl) and log(Vd) (natural logarithm of clearance and volume of distribution).
The residual variability was modeled with multiplicative error according to the following
equation:
𝑦𝑖𝑗 = 𝐶(θi , t ij , Di ) + 𝜀𝑖𝑗
th
Where Cij is the i measured plasma concentration for the jth patient; C(I,tij,Di) is the
expected plasma concentration from the model. ij is the residual variability term, representing
independent identically distributed statistical error with mean zero and variance 2 for serum
concentrations.
2.3.Bayesian stochastic model
2.3.1. Structure
Dataset of phenobarbital obtained from 59 subjects were analyzed by a one open
compartment model combined with 3 stage- hierarchical model.
Suppose we have a number (ni) of PK measurements made on each of K individuals, who
are indexed by i8. Denote the jth measurement for individual ith by yij and the associated time by
tij. Further, denote the p-dimensional vector of PK parameters for individual ith by I and the
residual error variance by 2.
The proposed stochastic model is:
1st stage: at the first of the three stages in our hierarchical model, we assume:
p(yiji,2) N(C(I,tij,Di), 2),
i = 1, 2…K.
j = 1, 2,…ni.
Where,
- yijs are either concentrations or log-concentrations the jth observation for the ith subject
depending on whether normality or log-normality is the more appropriate assumption for
the data.
- C(I,tij,Di): is the expected value of the data from the model.
- i is a vector of individual pharmacokinetic parameters for the ith subject.
2
2nd stage: At the second stage of the model, we make distributional assumptions regarding the
individual-specific PK parameter vector i. The model for between subject variability:
p(i , ) MVN p ( Zi , )
Where:
- MVN denotes a p-dimensional multivariate normal distribution.
- Zi is a pq covariate-effect design matrix for individual i.
- µ is a vector of q fixed effect parameters.
- Ω (pp) is the inter-individual variance-covariance matrix.
3rd stage: At the third stage of the hierarchical model, prior distributions are assigned to 2, µ
and :
p( 2 ) Inverse Gamma(a, b)
p( ) MVN q ( , )
p() IW ( R, )
Where;
- is a vector of prior population mean values of parameters
- is the prior variance matrix
- IW represents Inverse - Wishart distribution with parameters R and
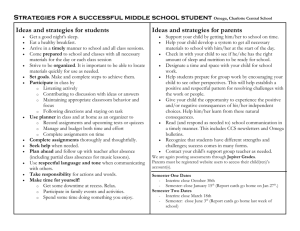
The structure of our model was built as figure below:
mu
om eg a
the ta i
Dose
PK mo de l
al p ha
Con c
si gma
for(j IN 1 : n i)
be ta
for(i IN 1 : K)
2.3.2. Priors
Informative prior
Making use of the knowledge which are means and coefficients of variance (%CV) of
clearance and volume of distribution gained from 4 studies of phenobarbital in neonates, prior
distributions of PK parameters of interest were constructed. In order to get the suggestion of
3
prior from WinBugs, weighted mean and %CV values of these parameters were calculated
following equations below and then entered in the program:
∑nj=1(Nj × μi,j )
)
E(θi =
∑nj=1 Nj
∑nj=1(Nj × Vari,j )
Var(θi ) =
∑nj=1 Nj
Once these values have been entered, the prior file should appear, in which the logtransformation was performed to provide the mean and variances according to these equations:
1
Var(θi )
E(logθi ) = ln(E[θi ]) − ln (1 +
)
2
E[θi ]2
Var(θi )
Var(logθi ) = ln (1 +
)
E[θi ]2
At the 3rd stage of the stochastic structure, prior distributions are assigned to 2, µ and
in the Prior document file, which are:
+ Prior for residual error: the residual is from many sources, including measurement error,
variability among laboratories, etc. Most of phenobarbital published studies do not include
information of residual errors. Thus, it is difficult to assign an informative prior for this factor.
As a results, non-informative prior which is G(0.001, 0.001) as PKBugs suggestion was chosen
for (equal to 1/2).
+ Prior mean of µ: mu.prior.mean = [E(logCl), E(logVd)]T
+ Prior precision matrix for µ (-1):
𝑉𝑎𝑟(𝑙𝑜𝑔𝐶𝑙)
0
Σ=[
]
0
𝑉𝑎𝑟(𝑙𝑜𝑔𝑉𝑑)
+ Prior inverse-omega matrix (-1): p(-1) = W(R, )
The value of R is set equal to (-p-1) multiplied by the initial estimate for the inter-individual
variability, in which is equal to equivalent prior sample size (approximately equal to total
number of subjects in 4 studies divided by 4 studies); is dimension of the matrix (in this case p
= 2).
( − p − 1) × 𝑉𝑎𝑟(𝑙𝑜𝑔𝐶𝑙)
0
𝑅= [
]
0
( − p − 1) × 𝑉𝑎𝑟(𝑙𝑜𝑔𝑉𝑑)
Non-informative prior
Assuming that we don’t have sufficient knowledge gained from literature, we will
continue to construct the model by using the suggested prior document which is generated by
PKBugs without editing it. For mu prior precision matrix (-1), the value of (logi) suggested by
PKBugs is 10-4. This choice is considered to ensure that the prior distribution for µ is both proper
and uninformative. For the value of R, PKBugs suggests setting the value of equal to p, to
obtain the least informative proper Wishart prior for -1.
2.3.3. Initial values
Three sets of initial values were generated for both the informative and uninformative
priors. One set was centered at the mean value of the parameters obtained from 4 previous
studies. One other set was over-dispersed initial values obtained from the initial estimates of
4
parameters equal to E(i)+2SD. The last set was under-dispersed generated from the initial
estimate of parameters which are equal to E(i)-2SD.
2.4.Implementation
The data were analyzed using PKBugs (version 1.1)/WinBUGS (version 1.3). PKBugs,
an add-on interface to WinBUGS was used to construct an object-oriented internal representation
of the model that is compatible with WinBUGS. Then WinBUGS 1.3.4 will be used to conduct
the remainder of the analysis in a normal way.
3. Results
3.1. Informative prior
Pharmacokinetics parameters in neonates from previous studies were tabulated in the
table below:
Table 1. Pharmacokinetic parameters of Phenobarbital in neonates
Ref
1
2
3
4
Clearance (ml/kg/h)
4.3 ± 1.1 (SD)
5.03 ± 31.9% (%CV)
4.7 ± 19% (%CV)
6.4 ± 35.9% (%CV)
Volume of distribution (L/kg)
0.71 ± 0.21 (SD)
1.09 ± 53.0% (%CV)
0.81 ± 0.12 (SD)
No of subjects
19
35
59
15
Based on the procedure of constructing informative priors in section 2.3.2, the following
values were obtained for clearance and volume of distribution parameters:
Table 2. Weighted mean and variance of PK parameters
Calculated value
E(i)
Var(i)
Inter-individual CV(%)
E(logi)
Var(logi)
Clearance
(ml/kg/h)
4.93
1.86
27.7
1.56
0.074
Volume of
distribution (L/kg)
0.92
0.19
47.4
-0.185
0.203
When the Done button was pressed, a WinBugs file named Priors appeared. This file
contains a (vague/non-informative) full prior specification for the analysis. From table 2, this
Priors document was edited as below to specify an informative prior for the model investigation.
tau.a = 0.001, tau.b = 0.001,
mu.prior.mean = c(
1.56,
-0.185),
mu.prior.precision = structure(
.Data = c(
1.35135, 0.0,
0.0,
0.49261),
.Dim = c(2, 2)),
omega.inv.matrix = structure(
.Data = c(
2.146, 0.0,
0.0,
5.887),
.Dim = c(2, 2)),
omega.inv.dof = 32.0
5
Realizing that after doing log-transformation, the variances of parameters of interest are
very low; in order to make the inter-variability among individuals more expected for a
population pharmacokinetics, we decreased the precision of logCl and logVd 10 times compared
to the calculated values.
3.2. Non-informative priors
For uninformative prior, we chose to analyze the prior generated by BKBugs 1.1 for the
model. After the initial estimates of PK parameters had been entered, a vague informative prior
was created:
tau.a = 0.001, tau.b = 0.001,
mu.prior.mean = c(
1.56,
-0.185),
mu.prior.precision = structure(
.Data = c(
1.0E-4, 0.0,
0.0,
1.0E-4),
.Dim = c(2, 2)),
omega.inv.matrix = structure(
.Data = c(
0.1496862082, 0.0,
0.0,
0.4192288198),
.Dim = c(2, 2)),
omega.inv.dof = 2.0
In this non-informative prior, degree of freedom in Wishart matrix was set equal to the
dimension of the matrix, which is 2 in this model.
3.3. Initial values for informative and non-informative priors
The numerical values for both priors were shown below:
Informative priors
Centered initial values
theta = structure(
.Data = c(
1.56,
-0.185,
1.56,
-0.185,
......)
tau = 1.0,
mu = c(
1.56, -0.185),
omega.inv = structure(
.Data = c(
14.91146319,
0.0,
0.0,
5.435705792),
.Dim = c(2, 2))
Over-dispersed initial values
list(
theta = structure(
.Data = c(
2.036011984,
0.5822156199,
2.036011984,
0.5822156199,
…………….)
tau = 1.0,
mu = c(
2.036011984,
0.5822156199),
omega.inv = structure(
.Data = c(
13.36128441,
0.0,
0.0,
4.770664386),
.Dim = c(2, 2))
6
Under-dispersed initial values
list(
theta = structure(
.Data = c(
0.7884573604, -2.995732274,
0.7884573604, -2.995732274,
……………………..)
tau = 1.0,
mu = c(
0.7884573604,
-2.995732274),
omega.inv = structure(
.Data = c(
13.36128441,
0.0,
0.0,
4.770664386),
.Dim = c(2, 2))
Initial values for non-informative priors
Similarly, 3 chains of initial values for non-informative prior investigation were obtained
and displayed in Appendix 2.
3.4. Estimation procedure
After loading priors and corresponding initial values, model code with data and three
chains of initial values were created and exported into WinBugs 1.4 to analyze. Below is the first
part of the generated code via PKBugs’ Export model:
model {
for (i in 1:n.ind) {
for (j in off.data[i]:(off.data[i + 1] - 1)) {
data[j] ~ dnorm(model[j], tau)
model[j] <- pk.model(1, theta[i, 1:p], time[j], hist[off.hist[i]:(off.hist[i + 1] - 1), 1:n.col], pos[j])
}
theta[i, 1:p] ~ dmnorm(theta.mean[i, 1:p], omega.inv[1:p, 1:p])
theta.mean[i, 1] <- mu[1]
theta.mean[i, 2] <- mu[2]
}
tau ~ dgamma(tau.a, tau.b)
sigma <- 1 / sqrt(tau)
mu[1:q] ~ dmnorm(mu.prior.mean[1:q], mu.prior.precision[1:q, 1:q])
omega.inv[1:p, 1:p] ~ dwish(omega.inv.matrix[1:p, 1:p], omega.inv.dof)
omega[1:p, 1:p] <- inverse(omega.inv[1:p, 1:p])
}
Convergence
During the analysis, 3 parameters including µ, and were monitored and updated
using Gibbs sampling. The model converged successfully after 20000 iterations. The history
plots indicate that mean values of 2 parameters start converge well at around 6000 iterations.
After that, all values are within a zone without strong periodicities and tendencies. Hence, 10000
first iterations were discarded for inference.
Kernel density plots were satisfactory because all of them look bell-shaped and
sufficiently symmetric.
It also can be seen that behavior of all of three chains looks the same in Gelman-Rubin
Diagnostic plots. After 10000 iterations, the red line starts stabilizing, in the mean while, two
blue and green ones becomes close together and horizontal.
7
Figure 1. History plots of µ, ,
mu[1] chains 1:3
5.0
2.5
0.0
-2.5
-5.0
-7.5
1
5000
10000
15000
20000
15000
20000
iteration
mu[2] chains 1:3
4.0
2.0
0.0
-2.0
-4.0
-6.0
1
5000
10000
iteration
omega[1,1] chains 1:3
0.4
0.3
0.2
0.1
0.0
10000
15000
20000
iteration
omega[1,2] chains 1:3
0.3
0.2
0.1
0.0
-0.1
10000
15000
iteration
8
20000
omega[2,1] chains 1:3
0.3
0.2
0.1
0.0
-0.1
10000
15000
20000
iteration
sigma chains 1:3
5.0
4.0
3.0
2.0
10000
15000
20000
iteration
Figure 2. Kernel density plots of µ, ,
mu[2] chains 1:3 sample: 48000
mu[1] chains 1:3 sample: 48000
6.0
omega[1,1] chains 1:3 sample: 48000
4.0
3.0
2.0
1.0
0.0
4.0
2.0
0.0
-6.0
-4.0
-2.0
15.0
10.0
5.0
0.0
0.0
-7.5
-5.0
-2.5
0.0
omega[2,2] chains 1:3 sample: 48000
2.5
0.0
sigma chains 1:3 sample: 48000
15.0
1.0
0.75
0.5
0.25
0.0
10.0
5.0
0.0
0.0
0.2
0.4
0.0
10.0
20.0
30.0
Figure 3. Gelman-Rubin Diagnostic plots of µ, ,
mu[1] chains 1:3
mu[2] chains 1:3
1.5
1.0
1.0
0.5
0.5
0.0
0.0
10050
12000
14000
10050
start-iteration
12000
start-iteration
9
14000
0.1
0.2
0.3
omega[1,2] chains 1:3
omega[1,1] chains 1:3
1.5
1.5
1.0
1.0
0.5
0.0
0.5
0.0
10050
12000
10050
14000
omega[2,1] chains 1:3
14000
omega[2,2] chains 1:3
1.5
1.5
1.0
1.0
0.5
0.0
0.5
0.0
10050
12000
start-iteration
start-iteration
12000
14000
10050
start-iteration
12000
14000
start-iteration
sigma chains 1:3
1.5
1.0
0.5
0.0
10050
12000
14000
start-iteration
Figure 4. Autocorrelation plots of µ, ,
mu[1] chains 1:3
mu[2] chains 1:3
1.0
0.5
0.0
-0.5
-1.0
1.0
0.5
0.0
-0.5
-1.0
0
20
40
0
20
lag
40
lag
omega[1,1] chains 1:3
omega[1,2] chains 1:3
1.0
0.5
0.0
-0.5
-1.0
1.0
0.5
0.0
-0.5
-1.0
0
20
40
0
20
lag
40
lag
omega[2,1] chains 1:3
omega[2,2] chains 1:3
1.0
0.5
0.0
-0.5
-1.0
1.0
0.5
0.0
-0.5
-1.0
0
20
40
0
lag
20
40
lag
10
sigma chains 1:3
1.0
0.5
0.0
-0.5
-1.0
0
20
40
lag
Regarding to the autocorrelation plots, the level of autocorrelation is higher for µ(1),
(1,1) and , which refers that these parameters in our model are more correlated compared to
others, so the Gibb sampler ran slower to explore the entire posterior distribution. However, after
40 lags, the level of autocorrelation was close to 0.2.
When compare the convergence of model with both priors, it can be seen that results
attained from sampling of non-informative prior are very similar to those from informative prior
(Figure 5, 6). The history, Gelman-Rubin diagnostic and autocorrelation plots all indicate that the
model also has good convergence. This result suggests that the prior does not have strong
influence on the posterior estimates. Respectively, data or likelihood was more influencing on
the posterior estimate from the model. Another reason may be possible which is the prior data
actually has a strong influence on the model fit, and the importance of using an appropriate set of
priors is observed. In particular, this conclusion is more confirmed in the poor posterior estimate
of parameters.
Figure 5. History plots of µ from non-informative prior
mu[1] chains 1:3
2.5
0.0
-2.5
-5.0
-7.5
1
5000
10000
15000
20000
15000
20000
iteration
mu[2] chains 1:3
4.0
2.0
0.0
-2.0
-4.0
1
5000
10000
iteration
11
Statistics
Sample statistics were obtained as below.
node
mu[1]
mu[2]
omega[1,1]
omega[1,2]
omega[2,1]
omega[2,2]
sigma
mean sd
MC error
-5.058 0.070570.001817
0.3644 0.061017.307E-4
0.1319 0.032579.268E-4
0.073850.0246 4.732E-4
0.073850.0246 4.732E-4
0.2017 0.032914.119E-4
2.82
0.2687 0.008769
2.5% median 97.5%
-5.196 -5.057 -4.918
0.2445 0.3642 0.485
0.078240.1284 0.2059
0.029910.072350.1268
0.029910.072350.1268
0.1473 0.1983 0.276
2.352 2.799 3.407
start
10000
10000
10000
10000
10000
10000
10000
sample
30003
30003
30003
30003
30003
30003
30003
MC error measuring the variability of each estimate due to simulation is low, so it can be
concluded that the calculation of the parameter of interest is highly precise. The mean and 95%
credible interval for all values of covariance between logCl and logVd do not include zero
value, which suggests that the substantial covariance was significant between these parameters.
Using non-informative prior, all values obtained are insignificantly different from
informative prior. Below is the results tabulated:
node
mu[1]
mu[2]
omega[1,1]
omega[1,2]
omega[2,1]
omega[2,2]
sigma
mean
-5.039
0.3485
0.2573
0.1754
0.1754
0.1844
2.706
sd
MC error
0.081570.001475
0.058385.585E-4
0.073880.00173
0.042975.785E-4
0.042975.785E-4
0.038714.663E-4
0.2289 0.004
2.5%
-5.201
0.2339
0.1401
0.1051
0.1051
0.1223
2.296
median 97.5%
-5.039 -4.88
0.3481 0.4636
0.2482 0.4275
0.1707 0.2723
0.1707 0.2723
0.1799 0.2745
2.692 3.19
start
10000
10000
10000
10000
10000
10000
10000
sample
30003
30003
30003
30003
30003
30003
30003
3.5.Model checking and sensitivity analysis
As George Box said that: “All models are wrong, some are useful”, checking the model is
crucial to statistical analysis. To analyze the sensitivity of our model, we investigated:
Effect of prior
After examining both informative and non-informative priors on the posterior
distributions, we noticed that there is no significant difference in posterior inferences from both
approaches. It may be due to sparse dataset obtained from previous studies. As the matter of fact,
our informative prior is not “informative” enough or inappropriate to create more accurate
posterior estimates. It is the common issue occurring in pediatric pharmacokinetic population
because of logistic and ethical reasons; it is improbable that intensive experimentation can be
carried out on each and every patient. So it can be observed that in the cases where the data are
informative, the model description of the data is reasonable even when it was fit using an
inappropriate set of prior data, thus indicating that the prior data has little influence in these
cases. But, in the case of less-informative data, the prior data has a strong influence on the model
fit. In particular, when the model was fit to the noninformative data using an inappropriate set of
prior data, the results will be poor7.
Covariate selection-issues in design and analysis
There are numerous challenges in design, conduct and analysis a population
pharmacokinetics studies in pediatric population. Populations in pediatric PK studies frequently
12
cover a much wider relative range in body size than comparable studies in adults. As a result, PK
parameters such as clearance, volume of distribution are usually functions of body size, such as
body weight, height and body surface area. In other word, body size is frequently highly
correlated with other development parameters such as renal function or volume of distribution.
Covariate selection becomes more sensitive in Bayesian analysis of pediatric phamacokinetic
population.
In this model, we chose no covariate analysis to estimate parameters. For this reason, it
should be considered as preliminary study. More sophisticated model could be constructed in
which proper covariates are added such as body size, gestational age, postconceptional age,
gender and apgar score. The lack of appropriate covariate incorporation into the model resulted
in deficiencies of this model for meaningful posterior inferences.
Comparison of posterior distribution to substantive knowledge
Based on the estimates of parameters logCl and logVd, we derived the results below:
Parameter
Clearance
Volume of distribution
Estimated log-value
-5.058
0.3644
Estimated value
6.4x10-3 (ml/kg/hr)
1.44 (L/kg)
The population mean of clearance was 6.4x10-3 (ml/kg/hr), which is not consistent with
those values obtained in previous pharmacokinetic studies. This value is extremely small and
looks wrong even thought the convergence of the model is pretty good.
The result of our data analysis indicated that the mean Vd of neonates treated with IV
bolus administration was 1.44 L/kg. It is higher than the value Vd/F of phenobarbital in neonates
which ranges from 0.7 to 1.2 L/kg 5 and 0.81 ± 0.12 l/kg in the work of Fischer et al3.
4. Conclusions
A 3 stage Bayesian hierarchical model was developed for fitting the dataset of
phenobartbital in 59 neonates after intravenous administration. Four previous studies of
phenobarbital in neonates and infants were used to construct an informative prior of the model.
After running 20000 iterations, the model converged successfully. However, no significant
difference in the results obtained from 2 informative and non-informative priors indicates that we
used inappropriate sets of prior. Hence, to improve the quality of model, more effective approach
of creating proper prior should be used7. In addition, after checking the model with substantive
knowledge and dealing with challenges of pediatric pharmacokinetic population, we concluded
that the inferences from the model could be more accurate if we incorporate into the model
potential effects of body size such as height, body surface area and other covariates. From
current literature, body size, age, apgar score are considered as statistically significant covariates
on the pediatric population model.
Appendix 1
Dataset obtained from: Grasela TH Jr, Donn SM. “Neonatal population pharmacokinetics
of phenobarbital derived from routine clinical data”. Dev Pharmacol Ther. 1985;8(6):374-83:
Neonatal pharmacokinetics of phenobarbital.
http://depts.washington.edu/rfpk/service/datasets/index.html
13
Due to the limited space of the project, a part of dataset containing information of first 10
subjects was displayed.
id
1
1
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
4
time
0
2
12.5
24.5
37
48
60.5
72.5
85.3
96.5
108.5
112.5
0
2
4
16
27.8
40
52
63.5
64
76
88
100
112
124
135.5
0
1.5
11.5
23.5
35.5
47.5
59.3
73
83.5
84
96.5
108.5
120
132
134.3
0
1.8
12
24.3
35.8
48.1
59.3
59.8
71.8
83.8
95.8
amt
25
.
3.5
3.5
3.5
3.5
3.5
3.5
3.5
3.5
3.5
.
15
.
3.8
3.8
3.8
3.8
3.8
.
3.8
3.8
3.8
3.8
3.8
3.8
.
30
.
3.7
3.7
3.7
3.7
3.7
3.7
.
3.7
3.7
3.7
3.7
3.7
.
18.6
.
2.3
2.3
2.3
2.3
.
2.3
2.3
2.3
2.3
weight
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.5
1.5
1.5
1.5
1.5
1.5
1.5
1.5
1.5
1.5
1.5
1.5
1.5
1.5
1.5
1.5
1.5
1.5
1.5
1.5
1.5
1.5
1.5
1.5
1.5
1.5
1.5
1.5
1.5
1.5
0.9
0.9
0.9
0.9
0.9
0.9
0.9
0.9
0.9
0.9
0.9
14
vargar
7
7
7
7
7
7
7
7
7
7
7
7
9
9
9
9
9
9
9
9
9
9
9
9
9
9
9
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
conc
.
17.3
.
.
.
.
.
.
.
.
.
31
.
9.7
.
.
.
.
.
24.6
.
.
.
.
.
.
33
.
18
.
.
.
.
.
.
23.8
.
.
.
.
.
24.3
.
20.8
.
.
.
.
23.9
.
.
.
.
4
4
4
5
5
5
5
5
5
5
5
5
5
5
5
5
5
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
8
8
8
8
8
8
8
8
8
8
8
107.8
119.8
130.8
0
2
12
24
36
48
59.5
60
72
84
96
108
120
132
0
1.8
11.8
23.8
35.8
47.8
59.3
59.8
71.8
83.8
95.8
107.8
120.1
131.8
142.8
0
2
11.3
23.3
36.5
48.2
60.3
73.8
75.8
84.3
96.3
108.3
120.3
132.3
144.5
165.3
0
1.7
11.8
23.7
35.7
47.7
59.7
71.7
73.7
83.7
95.7
2.3
2.3
.
27
.
3.4
3.4
3.4
3.4
.
3.4
3.4
3.4
3.4
3.4
3.4
.
24
.
3
3
3
3
.
3
3
3
3
3
3
3
.
19
.
2.4
2.4
2.4
2.4
2.4
.
2.4
2.4
2.4
2.4
2.4
2.4
2.4
.
24
.
3
3
3
3
3
3
.
3
3
0.9
0.9
0.9
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.2
1.2
1.2
1.2
1.2
1.2
1.2
1.2
1.2
1.2
1.2
1.2
1.2
1.2
1.2
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1.2
1.2
1.2
1.2
1.2
1.2
1.2
1.2
1.2
1.2
1.2
15
6
6
6
7
7
7
7
7
7
7
7
7
7
7
7
7
7
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
7
7
7
7
7
7
7
7
7
7
7
.
.
31.7
.
14.2
.
.
.
.
18.2
.
.
.
.
.
.
20.3
.
19
.
.
.
.
17.3
.
.
.
.
.
.
.
32.5
.
17.9
.
.
.
.
.
23.4
.
.
.
.
.
.
.
25.8
.
25.8
.
.
.
.
.
.
34.2
.
.
8
8
8
8
8
9
9
9
9
9
9
9
9
9
9
9
9
9
9
9
9
9
10
10
10
10
10
10
10
10
10
10
10
10
10
10
10
107.7
119.7
131.7
143.7
146.7
0
1.1
11.1
22.3
34.6
46.6
58.7
70.9
82.7
83.2
94.6
106.6
118.6
130.6
142.1
142.6
312.6
0
1.2
11.2
23.2
35.3
47.2
59.2
70.7
71.2
83.2
95.2
107.2
119.2
131.2
142.2
3
3
3
3
.
27
.
3.2
3.2
3.2
3.2
3.2
3.2
.
3.2
3.2
3.2
3.2
3.2
.
3.2
.
27
.
3.5
3.5
3.5
3.5
3.5
.
3.5
3.5
3.5
3.5
3.5
3.5
.
1.2
1.2
1.2
1.2
1.2
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
1.4
Appendix 2
Initial values for non-informative prior
Centered initial values
theta = structure(
.Data = c(
1.56,
-0.185,
1.56,
-0.185,
......)
tau = 1.0,
mu = c(
1.56,
-0.185),
omega.inv = structure(
.Data = c(
13.36128441,
0.0,
0.0,
4.770664386),
.Dim = c(2, 2))
16
7
7
7
7
7
8
8
8
8
8
8
8
8
8
8
8
8
8
8
8
8
8
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
.
.
.
.
36.1
.
22.1
.
.
.
.
.
.
29.2
.
.
.
.
.
34.2
.
19.6
.
19.9
.
.
.
.
.
23.4
.
.
.
.
.
.
30.9
Over-dispersed initial values
list(
theta = structure(
.Data = c(
2.036011984,
0.5822156199,
2.036011984,
0.5822156199,
…………….)
tau = 1.0,
mu = c(
2.036011984,
0.5822156199),
omega.inv = structure(
.Data = c(
13.36128441,
0.0,
0.0,
4.770664386),
Dim = c(2, 2))
Under-dispersed initial values
list(
theta = structure(
.Data = c(
0.7884573604, -2.995732274,
0.7884573604, -2.995732274,
……………………..)
tau = 1.0,
mu = c(
0.7884573604,
-2.995732274),
omega.inv = structure(
.Data = c(
13.36128441,
0.0,
0.0,
4.770664386),
.Dim = c(2, 2))
References
1. Touw D.J. et al, “Clinical pharmacokinetics of phenobarbital in neonates”. European
Journal of Pharmaceutical Sciences 12 (2000) 111–116.
2. E. Yukawa et al, “Population pharmacokinetic investigation of phenobarbital by mixed
effect modelling using routine clinical pharmacokinetic data in Japanese neonates and
infants”, Journal of Clinical Pharmacy and Therapeutics (2005) 30, 159–163.
3. Grasela TH Jr, Donn SM (1985) “Neonatal population pharmacokinetics of phenobarbital
derived from routine clinical data”. Developmental Pharmacology and Therapeutics, 8,
374–383.
4. Fischer JH, Lockman LA, Zaske D, Kriel R (1981). “Phenobarbital maintenance dose
requirements in treating neonatal eizures”. Neurology, 31, 1042–1044.
5. Battino D, Estienne M, Avanzini G (1995) “Clinical pharmacokinetics of antiepileptic
drugs in paediatric patients. Part I: phenobarbital, primidone, valproic acid, ethosuximide
and mesuximide”. Clinical Pharmacokinetics, 29, 257–286.
6. Heimann et al, “Pharmacokinetics of Phenobarbital in childhood”, Europ. J. clin.
Pharmacol. 12, 305-310 (1977).
7. Bernd Meibohm et al, “Population Pharmacokinetic Studies in Pediatrics: Issues in
Design and Analysis”, The AAPS Journal 2005; 7 (2).
8. David J. Lunn et al, “Bayesian Analysis of Population PK/PD Models: General Concepts
and Software”, Journal of Pharmacokinetics and Pharmacodynamics, Vol. 29, No. 3,
June 2002.
17