Viral Infections of the Skin
advertisement

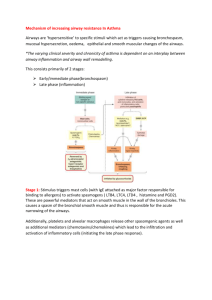
PBL CASE #3: FACULTY LEARNING ISSUES 1. (1) Describe the physiology and physics of airway resistance. Evaluate the respiratory work necessary to overcome airway resistance. Be sure you understand dynamic compression of airways. AIRWAY RESISTANCE As air flows through a tube, a difference in pressure exists between the ends and depends on the rate and pattern of flow. o Laminar flow: low flow rates, the stream lines are parallel to the sides of the tube The radius is of critical important when determining the resistance to flow through a tube o Transitional flow: as flow rate increases, unsteadiness develops, especially at branch points o Turbulent flow: at higher flow rate, complete disorganization occurs . In rapidly branching systems like the lungs, fully developed laminar flow likely only occurs in very small airways where the Re umbers are low. In most of the bronchial tree, the flow is transitional The major site of resistance in the medium sized bronchi o The very small bronchioles contribute relatively little resistance which is due to the vast number of small airways Factors determining airways resistance o Lung volume: as lung volume is reduced, airway resistance rise rapidly At low lung volumes, the small airways may close completely o Contraction of bronchial smooth muscle narrows airways and increases airways resistance May occur via reflexes (smoke) Stimulation of adrenergic receptors causes bronchodilation Parasympathetic activity causes bronchoconstriction (ACh) o Decreased PCO2 in alveolar gas causes an increase in airway resistance, as a direct action on bronchiolar smooth muscle o Histamine causes pulmonary artery constriction o Density and viscosity of gas affect resistance to flow Resistance in increased during a deep dive because the increases pressure raises gas density Reduced pressure when a helium-O2 mixture is breathed Dynamic Compression Airways Before inspiration has begun, airway pressure is zero everywhere. Because interpleural pressure is -5 cm H2O, there is a pressure of 5 cm H2O holding the airway open As inspiration begins, both intrapleural and alveolar pressure fall by 2 cm H2O and flow beings. Because of the pressure drop along the airway, the pressure inside is -1 cm H2O In each of the situations, the descending portion of the curve takes the same path, suggesting that something is limiting expiratory flow. dynamic compression of airway resistance Work required to overcome elastic forces Work overcoming the airway/tissue resistance During inspiration, the intrapleural pressure follows the curve A B C (work done by lung is the area 0ABCD0) 0ABCD0 = total work done by lung At end of inspiration, flow is zero and there is an airway transmural pressure of 8 cm H2O At the start of forced expiration, both intrapleural pressure and alveolar pressure increased by 38 cm H2O. Because of the pressure drop along the airway as flow beings, there is now a pressure 11 cm H2O and this closed the airway. Airway compression occurs and the downstream pressure limiting flow becomes the pressure outside the airway PBL CASE #3: FACULTY LEARNING ISSUES 2. A patient with asthma has an attack that results in bronchoconstriction to one lung lobe (drastically reducing its ventilation). Determine how this effects the VA/Q (ventilation –perfusion ratio) in that lobe and how does this effect the partial pressures of oxygen and carbon dioxide in the blood leaving that lobe and in the blood being delivered to the left ventricle? Be sure that you understand the mechanisms. With the bronchoconstriction and decreased ventilation form the asthma attack, there will be a decrease in the ventilation—perfusion ratio. A reduced VA/Q ratio is caused by obstruction in ventilation but blood flow is unchanged. As PO2 will decrease and PCO2 increase. With complete obstruction , the O2 and CO2 of alveolar gas and end-capillary blood must be the same as the mixed venous blood. Inspired Air: O2 = 150 and CO2 = 0 (A) Normal VA/Q ratio. The mixed venous blood entering has PO2 of 40 and PCO2 of 45. The alveolar PO2 of 100 is determined by balance between O2 addition via ventilation (PO2 inspired = 150) and its removal by blood flow. (B) Reduced VA/Q ratio (Asthma/COPD). This is caused by obstruction ventilation as blood flow is unchanged. When this happens alveolar PO2 will decrease and PCO2 increase. The relative changes are hard to calculate with partial obstruction. With complete obstruction, the O2 and CO2 of alveolar gas and end-capillary blood must be the same as the mixed venous blood. (C) Increased VA/Q ratio (PE): This is caused by obstruction of blood flow as ventilation is unchanged. In this situation, PO2 will increase and PCO2 will decrease, and the alveolar gas concentration will approach those levels of the inspired air. (2) PBL CASE #3: FACULTY LEARNING ISSUES With respect to asthma, describe its pathology, pathophysiology, and clinical presentation. PATHOLOGY Asthma is characterized by inflammation of the airway wall, with abnormal accumulation of eosinophils, lymphocytes, mast cells, macrophages, dendritic cells, and myofibroblasts. Inflammatory mediators and proteins secreted by these and other cells contribute directly and indirectly to changes in airway structure and function. The structural changes are found in both the epithelium and the submucosa, o abnormal deposition of collagen in the subepithelium o hyperplasia and/or hypertrophy of goblet cells, submucosal gland cells, smooth muscle cells, and blood vessel cells. Pathological changes seen in asthma o airway surface becomes more fragile o thickening of the epithelial reticular basement membrane o inflammation of the airways Presence of an inflammatory infiltrate made of activated T-cell and eosinophils. PATHOPHYSIOLOGY Inflammation o Airway inflammation is a key component of asthma and represents a complex interaction of inflammatory cells and airway cells o Proposed that individuals with appropriate susceptibility genes for asthma, when placed in a specific early life environment, develop a type of lymphocytic airway inflammation that results in asthma o Thus, naive T cells may be encouraged to differentiate toward a Th2 subtype. Secretion of typical Th2 cytokines such as IL-4, IL-5, and IL-13 in the airway promote eosinophilic and mast cell inflammation and structural airway changes typical of the asthma phenotype. The asthmatic airway inflammatory process, in which eosinophils, mast cells, and lymphocytes are abundant compared to normal subjects, is caused by the influence of TH2 cells, producing mediators including IL-3, IL-4, IL-5, IL13, and granulocyte-macrophage colony-stimulating factor (GM-CSF). Some of these mediators (IL-4) activate B lymphocytes to produce IgE or the mediated cause the continuation of eosinophilic airway inflammation (IL-3, IL-5, GM-CSF). Airway remodeling o Structural changes in the airway including include goblet cell metaplasia, deposition of collagens in the subepithelial space, hyperplasia of airway smooth muscle, and proliferation of submucosal glands. Results in thickening of the airway wall, and it involves both cartilaginous (large) airways and membranous (small) airways. CLINCIAL Associated with variable airflow limitations that are at least partly reversible either spontaneously or with treatment. Classic triad of symptoms o Persistent wheeze – 35 % o Chronic cough – 24 % o Chronic dyspnea – 29% Physical Exam: o Widespread, high-pitched wheezes (poor predictor of severity ) o Use of accessory muscles o Pulses paradoxus (greater than 10mmHg and fall in systolic pressure during inspiration) (3) 3. Immune mechanisms of asthma: antigen presentation to naïve CD4+ T cells by antigen-presenting cells (dendritic cells) causes either a Th1 or a Th2 response of CD4+ T cells Regulators of Th1/Th2 differentiation include IL-4, IL-10, and IL-12. Th2 cells secrete many different cytokines, which may or may not utilize inflammatory cells such as eosinophils, mast cells, and B cells as effectors. Airway remodeling in asthma is shown by healthy airway wall on the left and the asthmatic airway wall on the right. In asthma there is goblet cell hyperplasia/hypertrophy, subepithelial fibrosis, increased vascularity, and smooth muscle hypertrophy and hyperplasia. PBL CASE #3: FACULTY LEARNING ISSUES 4. If you evaluate an asthma patient with a battery of pulmonary function tests and give a rationale for your test selection and predict the results, what tests would you use and why? Expiratory Peak Flow Records airflow limitation by measuring the fastest rate of airflow during a forced expiration. The readings over a period of 1-2 weeks may be used to accurately diagnose asthma, estimate severity, and determine the response to treatment. Peak flow is also the best indicatory of response to therapy Spirometry measures forced expiratory volume in one second (FEV1) and forced vital capacity (FVC) The test is an accurate way to diagnose asthma and other airway diseases. With asthma and other obstructive lung diseases, the lungs fill up easily, but cannot empty. o TLC is normal o FRC, RV are increased o VC, FEV1, FEV1/VC% are decreased In comparison, with a restrictive lung disease, the lungs are less compliant than normal o TLC, IC, VC are decreased o RV is normal o FEV1/VC% is normal or increased 5. Upon Mr. Vu’s initial evaluation, do you feel his problem was miss managed? If so, why? Prior to this doctor visit, Mr. Vu was prescribed theophylline and an inhaled steroid for his asthma therapy; he also had a PRN prescription for an inhaled Bagonist (albuterol). Based on his condition when he visited the clinic, it is obvious that his care was mismanaged. From Mr. Vu’s history, no information was provided concerning previous peak flow meter tests to determine the severity of asthma (mild intermittent, mild persistent, moderate persistent, and severe). o Based on his current symptoms, and his previous hospitalization for asthma, Mr, Vu would be either in the moderate persisitant or severe category. Based upon this evaluation, his therapy should have included a B-agonist inhaler PRN + an inhaled steroid + a leukotriene inhibitor and/or long acting beta agonist. In addition, Mr. Vu likely suffers from Samter’s Traid, which is characterized by the clinical triad of asthma, nasal polyps and aspirin sensitivity (late). o Treatment: Nasal steroids/inhaled steroids, and leukotriene antagonists (which is the same as indicated for his asthma treatment). Surgery can be done to remove polyps, although they typically recur. Mr. Vu also needs to be properly educated on how to use the inhalers. Theophylline was a controversial choice, as it is not indicated in first line asthma treatment. Theophylline also has not been indicated to be greatly beneficial and has toxicities and narrow therapeutic index. (diuretic effects, CNS stimulation) (4) PBL CASE #3: FACULTY LEARNING ISSUES (5) 6. Compare and contrast recommended drug regimens for pure asthma vs COPD. COPD Treatment o Smoking cessation Slows decline in FEV-1 o Asthma Therapy β-2 agonist bronchodialators Metered dose inhaler o Anticholinergic Agents Inhaled ipratropium – first line therapy Additive effects of anticholinergics and beta-agonists o Theophylline Use is controversial; watch for toxicity (very narrow therapeutic index.) o Corticosteroids Inhaled –may slow rate of decline of FEV-1 Oral – up to 20% of patients may benefit Consider short term use for exacerbations Long term use only if all other meds are at maximal therapy o Supplemental Oxygen If O2 saturation < 88% on room air or < 85% with exertion Asthma Treatment o Mild intermittent: β -agonist inhaler PRN. o Mild persistent β -agonist inhaler PRN. + inhaled steroid o Moderate persistent β -agonist inhaler PRN. + inhaled steroid + leukotriene inhibitor and/or long acting beta agonist o Severe Multiple controller meds Consider oral steroids. 7. Discuss patient education and involvement in his/her own treatment of chronic lung disease. Discuss the issue of patient compliance with drug regimens and monitoring PEFR. Low rates of patient compliance pose a major challenge to effective asthma management. Non-compliance depends on many factors o patient's own treatment goals o social and economic factors o administration route o convenience of device o side-effects Poor patient compliance may also be due to a discrepancy between the goals of the clinician and those of the patient. Clinicians tend to focus on prevention of mortality and reduction of morbidity, PEFR rates takes an home by the patient are the most effective way at self monitoring and control of asthma symptoms. o Peak expiratory flow rates “Red” – less than 50% of personal best Emergency situation for patient – may need oral steroids “Yellow” – 50 to 80% Patient may need to take additional asthma meds may to control worsening symptoms “Green” – Over 80% Asthma under control and patient just needs to track what medications were taken that day 8. Know the mechanism of aspirin-induced PBL CASE #3: FACULTY LEARNING ISSUES (6) hypersensitivity and the potential of cross-reactivity with any NSAID. 9. The etiology of aspirin sensitivity is unknown but believed that the disorder is caused by an disorder in the arachidonic acid cascade increased production of leukotrienes o Mechanism 1: Blockade of COX shifts arachidonate utilization to the lipoxygenase pathway. The end result is increased leukotriene production and the symptoms of hypersensitivity. Upregulation of the Cys LTR1 is also seen. o Mechanism 2: Inhibition of COX 1 decreased synthesis of PGE2. Removing this PGE2 eliminates its critical blocking effect on 5-lipoxygenase, allowing rapid synthesis of leukotrienes. This increase in leukotrienes leads to delayed mast cell degranulation with a subsequent release of histamine. Aspirin is the dominant cause and other cyclooxygenase inhibitors can cause it also. People with aspirin sensitivity can have cross-reactivity to other non-steroidal anti-inflammatory compounds such as ibuprofen and naproxen o Even some documented cross-reactivity with acetaminophen. But there is no cross-reactivity with selective cyclo-oxygenase 2 inhibitors. Describe the proper use of an inhaler. Is nebulizer as a treatment more effective than an inhaler? MDI W/O SPACER (Albuterol/Combivent) Remove the cap from the mouthpiece and shake the inhaler Breathe out to the end of a normal breath, position the mouthpiece end of the inhaler about 2-3 finger widths from mouth. Close your lips around the mouthpiece and start to breathe in slowly Push down once on the container; this will spray medication into mouth. Continue breathing in slowly until lungs are full Once a full breath is reached, hold breath for 10 seconds or as long as possible, then breathe out normally If a second puff needed, wait one minute and repeat steps. MDI W/ SPACER (Albuterol/Combivent) Remove the cap of the inhaler and shake well Insert the inhaler in the inhaler adaptor at the back of the spacing chamber Exhale as much as possible until lungs feel empty. Seal lips around the spacing mouthpiece Press down once on the inhaler's container, which will spray medication into the chamber Breathe in slowly and deeply Once breathed in fully, hold breath for 10 seconds or as long as possible, then exhale normally USE OF DISK INHALER (Advair) Seal lips around the mouthpiece. Inhale rapidly and deeply. Continue to take a full, deep breath. Hold breath for up to ten seconds. This allows the medication time to deposit in the airways. Resume normal breathing NEBULIZER VS. MULTIPLE DOSE INHALER (MDI) Research comparing efficacy of nebulizers and MDI has shown no difference between the two treatment groups with regard to hospital admission rates. However, the use of the MDI with spacer provided greater improvement in peak-flow rates than use of the nebulizer. MDI users had a lower total albuterol dose and showed greater improvement in arterial blood gases. Asthma relapse rates were significantly lower for the MDI users than for nebulizer users treated by nebulizer. Mechanism of Aspirin Sensitivity: blockage of the COX pathway causes a shift to the LOX pathway leading to an increase production of leukotrienes mast cell degranulation histamine release bronchoconstriction PBL CASE #3: FACULTY LEARNING ISSUES (7) Class 1st generation antihistamine Mechanism Block H1, muscarinic, adrenergic, and serotonin receptors Distribution Oral, widely distributed (CNS) Elimination Transformed in liver, excreted in urine Fexofenadine 2nd generation antihistamine Loratidine 2nd generation antihistamine Theophylline Methylxanthine; bronchodilator Cromolyn sodium Anti-asthma; mast cell destablizer Oral, does NOT enter CNS Oral, does NOT enter CNS Oral, wide availability Poorly absorbed, inhalation only Transformed in liver, excreted in urine Transformed in liver, excreted in urine Metabolized by liver, excreted by kidney N/A nedocromil Anti-asthma; mast cell destablizer Adrenergic agonist; bronchodilator, alpha-1, β1, β2 Block H1, muscarinic, adrenergic, and serotonin receptors Block H1, muscarinic, adrenergic, and seratonin receptors Antagonists of adenosine receptors, ↓ histamine release, bronchodilation ↓ histamine release, reduction in bronchospasms (no relaxation of smooth muscle), value when taken prophylactically inhibits the release of histamine from mast cells Relaxes the bronchioles via β2 activation, used in anaphylaxis Poorly absorbed, inhalation only Inhalation/injection Not metabolized, eliminated by kidney Metabolized rapidly in liver my COMT/MOA, kidney elimination Releases norepinephrine and causes bronchiole relaxation by direct effect Bronchiole relaxation, inhibits mast cell degranulation Oral administration Diphenhydramine Tripelennamine Chlorpheniramine Hydroxyzine Promethazine Epinephrine Ephedrine Sympathomimetic, adrenergic Metaproterenol β2 agonist, bronchodilator Metabolized in GI tract Terbutaline Poor oral availability, Inhalation Inhalation/IV Albuterol/Salbutamol Inhalation Kidney elimination Inhalation Hepatic metabolism/fecal elimination P450 metabolism (watch for hepatic toxicity) Hepatic metabolism, fecal elimination Hepatic metabolism, fecal elimination Salmeterol Long acting Zilueton Leukotriene Inhibitor Phenylephrine α1 agonist, decongestant Inhibits 5-lipoxygenase and prevents formation of LTB4 (chronic asthma) Leukotriene receptor antagonist (LTD4 receptor) Leukotriene receptor antagonist (LTD4 receptor) Constriction of vasculature Pseudoephedrine Sympathomimetic, adrenergic agonist Glucocorticoid; anti- Releases norepinephrine and causes bronchiole relaxation Inhibits inflammatory cells and release Zafirlukast Montelukast Betamethasone Oral availability Oral administration Oral availability Oral availability Kidney elimination Oral availability Inhalation/nasal Metabolized in liver, excreted Side Effects Low incidence of GI side effect, ↑ sedation, used for motion sickness GI side effects common, few CNS effect, fewer anticholinergic effects No sedative effects, good for day time use Sedation (↑), longer lasting, potentially teratogenic Used as anti-psychotic/anti-emetic, ↑ anticholinergic effects, used for motion sickness (antichol effect) Minimal anticholinergic effect, NO sedation Minimal anticholinergic effect, NO sedation Insomnia, nervousness, arrhythmias, GI bleeding, vomiting Sore throat, cough, dry mouth, nausea, headache Cough, bad taste in mouth, nausea/vomiting, headache Arrhythmia, tachycardia, sweating, nausea/vomiting Hypertenstion, palpitations, nausea/vomiting Muscle tremors, nervousness, palpitations Muscle tremors, nervousness, palpitations Muscle tremors, nervousness, palpitations Long acting, tachycardia, headache, tremor P450 drug interactions; diarrhea, indigestion, headache, vomitting Inhibits P450, many drug interactions Inhibits P450, many drug interactions Hypertension Hypertension, tachycardia, insomnia, anxiety Immunosuppresion (long term PBL CASE #3: FACULTY LEARNING ISSUES Dexamethasone (8) inflammatory steroid of inflammatory mediators. Class Glucocorticoid; antiinflammatory steroid Mechanism Inhibits inflammatory cells and inhibits release of inflammatory mediators. (decrease arachidonic acid release, dec degranulation of mast cells)..inhibits phospholipase A2 spray, can have some systemic distribution Distribution Orally available. Careful with abrupt cessation b/c person shut off synthesizing own steroids Methylprednisolone Orally available Prednisone Orally available Triamcinolone Orally available, inhalation Beclamethasone Inhalation/nasal spray, can have some systemic distribution Flunisolide Inhalation/nasal spray, can have some systemic distribution Inhalation/nasal spray, can have some systemic distribution Bedesonide Fluticasone Inhalation/nasal spray, can have some systemic distribution by kidney Elimination Metabolized in liver, excreted by kidney usages, headache, most anti-inflam. along with dexamethasone Side Effects Immunosuppresion (long term), headache, oral candidiasis (thrush), dysphonia, hoarseness, reflex cough and bronchospasm, (systemic: weight gain, fluid retention, elev blood sugars, osteoporosis, growth suppression, cataracts…same with all systemic glucocort..for severe asthma)..bolded are main ones for glucocort. Immunosuppresion (long term), headache, oral candidiasis (thrush), dysphonia, reflex cough and bronchospasm Immunosuppresion (long term), headache, oral candidiasis (thrush), dysphonia, reflex cough and bronchospasm Immunosuppresion (long term), headache, oral candidiasis (thrush), dysphonia, reflex cough and bronchospasm Immunosuppresion (long term), headache, oral candidiasis (thrush), dysphonia, reflex cough and bronchospasm, fewer side effects Most potent of steroids, fewer side effects, nasal irritation Immunosuppresion (long term), headache, oral candidiasis (thrush), dysphonia, reflex cough and bronchospasm Immunosuppresion (long term), headache, oral candidiasis (thrush), dysphonia, reflex cough and bronchospasm, nasal irritation