Dolphin_&_Hennessy_(2014)_Psychiatry_Research
advertisement
_Psychiatry_Research")
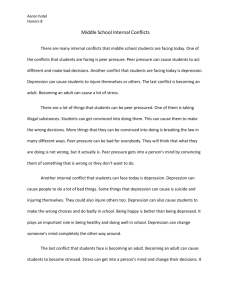
Adolescents' perceptions of peers with depression: an attributional analysis Louise Dolphin, Eilis Hennessy* University College Dublin, School of Psychology, Dublin, Ireland *Corresponding author Address: School of Psychology, Newman Building, UCD, Belfield, Dublin 4, Ireland Telephone Number: +353 1 716 8362 Email Address: eilis.hennessy@ucd.ie 1 Abstract Understanding adolescents' perceptions of peers with depression is vital in order to tackle peer exclusion and lessen stigmatization. To examine adolescents' perceptions of a hypothetical peer with depression, we test an attributional model: that stigma towards persons with mental disorders is influenced by attributions about the causes of their disorders and inferences of personal responsibility. Participants were 401 adolescents from 4th year/10th grade with an age range of 14.75-17.08 years (M=15.90 years; SD=0.403 years). Structural Equation Modeling was employed to assess the relationships among causal attributions (personal control), perceived responsibility, and emotional reactions, in predicting social acceptance/exclusion of a peer with depression. Results indicated that (a) if the peer with depression is perceived as having little control over the cause of depression, responsibility is not inferred, participants feel sympathy and pity, and are likely to socially accept the peer (b) gender of vignette character and participant influence these responses. This study builds on our theoretical understanding of why adolescents with depression may face social exclusion from peers by applying a well‐established theory in social psychology. Findings should be incorporated into the design of interventions aimed at reducing peer exclusion and stigmatization of adolescents with depression. Key words: depression; adolescence; peer group; attribution theory; SEM 2 1. Introduction 1.1. Adolescent depression and the peer group Adolescent depression is receiving increasing attention in the psychological literature, which is unsurprising considering the prevalence rates reported in many studies. Lewinsohn et al. (1998) estimated that approximately 28% of adolescents will have experienced an episode of Major Depressive Disorder by the age of 19. Ireland's first comprehensive national study of youth mental health indicates that 30% of Irish adolescents score outside the normal range for depression (Dooley and Fitzgerald, 2012). Both studies indicate higher rates of depression for female adolescents. However, very few studies have investigated the factors that predict the social acceptance or exclusion of adolescents with depression by their peer group. Social exclusion is linked to discrimination- a key aspect of the stigmatization process (Link and Phelan, 2001). This lack of focus is surprising given that research indicates that the peer group can offer some protection from depressive affect in adolescence (La Greca and Moore Harrison, 2005; Steinhausen and Metzke, 2001). Social exclusion from the peer group (i.e. peer exclusion) can take the form of exclusion from activities, being ignored, or receiving a lack of attention from peers. This type of peer exclusion is a significant predictor of emotional distress in adolescence (Kenny et al., 2013). Additionally, adolescents experiencing symptoms of depression experience decreased acceptance and support from their peers (Stice et al., 2004) and the reasoning behind this is currently poorly understood. To understand the factors that predict peer acceptance or exclusion, a strong theoretical model must be employed. However, research in this area is lacking in theoretically driven studies. One potentially powerful model which could be employed to address this gap is Attribution Theory (AT; Weiner, 1985), a well established theory in social psychology. 1.2. Attribution theory Attribution theory is a theory of social cognition which has been utilized to explain responses to people with mental disorders (Corrigan et al., 2003; Martin et al., 2000; Weiner et al., 1988). In essence, AT links the underlying structure of our causal thinking to the dynamics of emotions and actions (Weiner, 1985). In its simplest form, AT hypothesizes that people make causal attributions about the behavior of others, these causal attributions give rise to emotions, and these emotions guide reactive behavior (Weiner 1985, 1986). A simple example is as follows. If somebody crashes into your car and you learn that they were texting on their mobile phone, you are likely to perceive the cause of the crash as controllable, you feel angry, and you react to the other person with annoyance. On the other hand, if you learn that the person who crashed into your car had a heart attack and lost control of their vehicle, you are more likely to perceive the cause of the crash as uncontrollable, and you experience sympathy which is likely to result in you providing assistance. Weiner (1985, 1986) proposed various dimensions of causal attribution (locus, controllability, stability), but Anderson and Arnoult (1985) argued that 'personal control' (whether a cause is perceived by the attributor to be under volitional control) is the most important causal dimension. Weiner (1988) highlighted that the key aspect of the attribution model is the mediating role of emotions as determinants of an individual's subsequent behavior (e.g. social 3 acceptance/exclusion). In particular, emotions of anger and pity are thought to influence behavior towards others. Research has provided evidence that the perception of controllability is the main causal dimension linked with these emotions (Meyer and Mulherin, 1980; Weiner et al., 1982). Anger is greater in the case of controllable causes, whereas pity is greater when the cause of behavior is perceived as uncontrollable (Weiner et al., 1982). Weiner (1993) argued that when reacting to stigmatized individuals, observers/attributors search for causation, and also judge personal responsibility. Whilst causal controllability is a major determinant of responsibility, they differ in that controllability is a causal property, whereas responsibility is an inference or judgment about a person (Weiner, 1993; 1995). Sometimes cause is located within the person and is controllable, but still responsibility is not inferred e.g. a business failure due to caring for a sick relative (Weiner, 1995). Therefore, in incorporating responsibility into AT, Weiner (1993) proposed a sequence whereby personal control predicts inferences of responsibility, which influences emotional reactions, and these emotional reactions predict behavior. 1.3. Attribution theory and peer exclusion Juvonen (1991) showed that sixth grade students rate certain types of "deviant" peers more negatively than others, depending on the level of responsibility attributed to the behavior. For example, children perceived bragging and aggressive peers as more responsible for their behavior and thus they evoked more negative emotions (anger and irritation) than peers who were socially withdrawn, or had a physical condition. In line with AT, Juvonen concluded that the more a peer induced positive emotions (sympathy and pity), the more likely children were to support them. Conversely, the more a peer elicited negative emotions (anger and irritation), the more likely they were to be excluded. In terms of depression, there is evidence that children rate a depressed peer with high life stress more positively than a depressed peer with low life stress (Peterson et al., 1985). In other words, attributing depression to external stress reduces the tendency to act negatively towards a depressed peer. If attributions of personal control over the cause of a disorder can influence subsequent behavior, this may have implications for the design and implementation of anti-stigma interventions. 1.4. Gender differences Reported rates of depression increase more steeply for girls than boys during adolescence. Nolen-Hoeksema and Girgus (1994) claim that after the age of 15, girls are about twice as likely to be depressed as boys, indicating that mid-late adolescence is a key time to investigate gender differences in adolescent responses to peers with depression. Research has also highlighted that adolescents have differential attitudes towards male peers with mental disorders and female peers with mental disorders. In light of AT, recent research indicates that greater belief in a child’s responsibility for his condition (ADHD or depression) is associated with lower acceptance for males only (Swords et al., 2011). The authors suggest that further work is necessary to investigate why attributions of responsibility have a greater influence in judgments of boys in comparison to girls. Although participants in the Swords et al. (2011) study responded to both male and female hypothetical peers, the majority of studies examining perceptions of aggression and withdrawal have used only males as the stimuli (e.g. Juvonen, 1991; 4 Peterson et al., 1985; Sigelman and Begley, 1987). This has left gaps in the literature in terms of our understanding of the effect the vignette character's gender has on responses. 1.5. The present study We employ a strong theoretical framework by applying a fuller model of AT than has been previously used, to test adolescents' causal attributions of personal control, inferences of responsibility, emotional reactions, and peer acceptance of a hypothetical peer presented as clinically depressed. Our study builds on previous research in several ways. Much of the mental health literature is based on adolescents' understanding of mental disorders as general concepts rather than how they understand specific symptoms (e.g. feeling anxious) which may represent preliminary manifestations of more serious mental health difficulties (MacLean et al., 2012). Therefore the vignette in this study focuses on specific symptoms of depression without explicitly labeling it. Unlike previous research that has explored this issue from an attributional perspective, this study does not provide participants with information regarding the cause of the depressed behavior; rather, they will be asked to suggest a possible cause of such behavior. This method of using a freeresponse procedure was deemed as an appropriate research procedure by Weiner (1985). In addition, McAuley et al. (1992) criticized research in the area of AT for translating participants' causal attributions into the causal dimensions and therefore committing the fundamental attribution research error. In other words, previous research assumed that the researcher and participant perceived causes in the same way (for example, assuming that all people view genetic causes as low on personal control and environmental causes as higher on personal control). To avoid this, this study asks participants to explicitly indicate the level of personal control they attribute to their suggested cause of depression. Consistent with previous attribution research (Juvonen, 1991; Weiner, 1993; Weiner et al., 1988), our study hypothesizes that causes of depressive behavior perceived as uncontrollable will not elicit inferences of responsibility, pity/sympathy will be elicited, and this will result in peer acceptance. Conversely, when the cause of depressed behavior is perceived as controllable, inferences of responsibility and the emotion of anger/irritation will be elicited, which will result in peer exclusion. 2. Method 2.1. Participants Participants were 401 adolescents with an age range of 14.75-17.08 years (M=15.90 years; SD=0.403 years). The gender distribution of the sample was 53.1% female (n=213) to 46.9% (n=188) male. Adolescents were recruited from fourth year (students in their 12th year of school). These adolescents were recruited from ten, non fee paying, single sex secondary schools, selected from schools with 600+ students on the Irish Department of Education published lists of schools in SouthEast Ireland. Following ethical approval, 23 secondary schools in the Republic of Ireland were contacted. The response rate from schools was 44%. Students were asked to bring information sheets and consent forms home to their parents and to bring back in the consent form, signed, on the arranged date of data collection if they wished to participate. The information sheet described 5 the research as a study of peer relationships and mental health in adolescence. Only students who returned signed parental consent forms were included in the study. 2.2. Ethical approval Ethical approval for this study was granted from the Human Research Ethics CommitteeHumanities of University College Dublin (Research Ethics Reference Number: HS-11-31). 2.3. Materials 2.3.1. Questionnaire Participants completed a hardcopy questionnaire consisting of their responses to a vignette/short description of a hypothetical peer with depression. 2.3.2. Vignettes The vignette (see Appendix A), developed by the author, was based on previous, similar research, describing an adolescent with symptoms of depression. Half of the sample responded to a female vignette character and the other half responded to a male vignette character. Symptoms were based on DSM-IV (American Psychiatric Association, 1994), ICD-10 (WHO; 1992) and Achenbach’s (1991) Child Behavior Checklist criteria. The vignette was sent to accredited clinical psychologists (n=5) for validation and suggestions for improvement were given (e.g. "he/she rarely replies to texts or signs onto Facebook chat or MSN") and incorporated into the final vignette. Participants were asked to respond to the vignette by completing the measures and items below. 2.3.3. Causal attributions Participants completed the personal control subscale of The Revised Causal Dimension Scale (CDSII; McAuley et al., 1992), adapted to refer to third person rather than self attributions (as done in previous research e.g. Jones and Hastings, 2003). This subscale consists of three items, each rated on a 9-point scale. Participants wrote down what they thought was the most likely cause of the behavior described in the vignette and rated this cause in terms of personal control. The original CDSII scale has good construct validity and internal consistency (McAuley et al., 1992). Previous research with adults (Jones and Hastings, 2003) indicates that adapting this measure to the third person does not affect the psychometric properties of the scale. In our study, the internal consistency of personal control subscale was α=0.74. 2.3.4. Perceived responsibility and emotional reactions Based on Juvonen's (1991) methodology, participants were asked two items relating to perceived responsibility and four items about how the hypothetical peer's behavior made them feel. Two of these items related to positive emotions (sympathy and pity) and two items related to negative emotions (irritation and anger). Participants answered these six questions on 6-point scales, and three of the six items were reverse scored. 2.3.5. Peer acceptance 6 The Friendship Activity Scale (FAS; Siperstein, 1980) is a 17-item scale, developed to assess a child or adolescent's desire to engage with a peer in social, academic and general activities. It is widely used to gauge behavioral intentions, particularly in a school context. Each statement is followed by a four-point scale to rate whether the participant would engage in the activity with a peer. Following a pilot study, the original FAS was modified to make the items more developmentally appropriate for the adolescent sample used in this study. Five items were deleted and minor wording changes were made to several items (e.g. "play with" was changed to "hang around with"). Therefore, the modified measure consisted of 13 items pertaining to adolescents' acceptance of the vignette character across a range of activities. Scores ranged from 13 (most negative) to 52 (most positive). Internal consistency was very good (α=0.83). 2.4. Procedure Data collection took place during school hours and the questionnaire took approximately 30 minutes to complete. To enhance confidentiality, sections of the questionnaire were randomized; therefore participants were rarely on the same section as the student next to them. Participants were asked not to write their name on the questionnaire. Following completion, the researcher collected and stored the questionnaires and consent forms securely and separately. 3. Results Structural equation modeling was used to model the relationships between causal attributions of personal control, responsibility, positive emotions, negative emotions, and peer acceptance. All statistical analyses were conducted using AMOS version 18. 3.1. Structural equation modeling (SEM) analyses The goal of this study was to investigate the relationships among causal attributions of personal control, responsibility, positive and negative emotions, and peer acceptance of a vignette character presented as depressed, and to test whether adolescents respond differently to male and female vignette characters. Table 1 presents means, standard deviations, and factor loadings for each of these items. Measured variables which did not load significantly onto their respective latent variables were not retained. Therefore, one responsibility item was removed from both models and one anger item was removed from the female vignette model. INSERT TABLE 1 The model was defined a priori (see Figure 1). Two models were tested, splitting the sample based on the gender of the vignette character they responded to. All reported statistics reflect within model observations. INSERT FIGURE 1 Decisions regarding model fit were based on the root mean square error of approximation (RMSEA) with a 90% confidence interval, the Comparative Fit Index (CFI), and the Incremental Fit Index (IFI). Though there has been much debate around the appropriateness of looking to chi-square results, chi-square is deemed to be acceptable if the ratio of the chi-square to the degrees of freedom is between two and five (Bollen and Long, 1993). Model fit was determined based on the 7 criteria that RMSEA between 0.05 and 0.08 indicates acceptable fit, and IFI and CFI above 0.90 indicate acceptable fit (Browne and Cudeck, 1993). Model A (male vignette character; see Figure 2) indicated relatively good fit. Whilst the CFI (0.742) and IFI (0.757) were below the recommended fit of 0.90, the RMSEA of 0.073 indicated that the model fitted the data well and the ratio of chi square to degrees of freedom was 2.04, which indicated acceptable fit. Model B (female vignette character; see Figure 3) also fitted the data well, yielding a CFI of 0.810, IFI of 0.818, RMSEA or 0.074, and chi square to degrees of freedom ratio of 2.09. In model A (male vignette character; see Figure 2), all hypothesized relationships and regression pathways predicted by attribution theory were significant with the exception of negative emotions/peer acceptance. Attributions of personal control over the cause of the depressed behavior, positively predicted inferences of responsibility (β=0.40, p < 0.001). In turn, inferences of responsibility positively predicted negative emotions of anger (β = 0.31, p < 0.05), and negatively predicted positive emotions of sympathy (β=-0.28, p < 0.05). Finally, positive emotions predicted social acceptance (β=0.50, p < 0.01). Participant gender significantly impacted on attributions of personal control, with males attributing more personal control over the cause of depression than females within this model (β=-0.20, p < 0.05). INSERT FIGURE 2 In model B (female vignette character; see Figure 3), personal control over the cause of depressed behavior positively predicted inferences of responsibility (β=0.49, p < 0.001). While responsibility negatively predicted emotions of sympathy (β=-0.23, p < 0.05), a significant relationship was not observed between responsibility and anger. Anger did not significantly predict peer acceptance, but positive emotions positively predicted peer acceptance (β=0.43, p < 0.01). In terms of participant gender within this model, females showed greater acceptance of a female vignette character than males (β=0.20, p < 0.05). INSERT FIGURE 3 4. Discussion 4.1. Summary findings This study employed Structural Equation Modeling to test the pathways predicted by attribution theory (AT; Weiner, 1985, 1986, 1993, 1995) separately for male and female adolescents with depression. Our findings suggest that peer acceptance of both male and female adolescents with depression is predicted by pathways whereby cause of depression is perceived as uncontrollable, responsibility is not inferred, and sympathy/pity is felt by the participant. These findings are consistent with the theoretical framework of AT. Relationships among other variables vary as a function of the gender of the adolescent with depression, and the participant's gender. All but one theoretical pathway is significant when participants respond to a male vignette character with depression. Alongside the above findings, the male character elicited responses whereby inferences of responsibility predict emotions of 8 anger/irritation. However, these emotions do not predict peer exclusion. In terms of participant gender, males view other males as having more personal control over the cause of depression. On the other hand, the theoretical pathway between responsibility and anger is not significant when the peer with depression is female. Additionally, a significant pathway between anger/irritation and peer exclusion was not observed. In terms of participant gender, female gender predicted social acceptance of a female peer with depression. 4.2. Theoretical implications In line with previous research with children (Juvonen, 1991), we found the mediating role of emotions in an attributional model (Schmidt and Weiner, 1988) to be important, with the link between responsibility and anger playing a more significant role in adolescent responses to male peers with depression than to female peers. Contrary to the tenets of AT, neither of the models tested found a significant relationship between anger/irritation emotions and peer exclusion. However, this has been the case in previous research; Juvonen (1991) found that children's negative emotions did not predict willingness to provide social support for a hypothetical peer. This could mean one of two things. On one hand adolescents could feel angry towards depressed behavior in a peer but do not let this anger influence their acceptance/exclusion of the peer. On the other hand, the absence of the negative emotion/peer exclusion link could be explained by social desirability; i.e. an adolescent may feel angry or irritated by depressed behavior in a male peer but will not admit that they would act out or socially exclude the peer based on this anger. This study builds on previous research by using a free-response procedure regarding the cause of the depressed behavior, and, by asking participants to explicitly rate the level of personal control they attribute to that cause, avoiding the fundamental attribution research error (see Section 1.5). To our knowledge, such a rigorous theoretical assessment of AT has not been previously conducted to understand adolescents' causal thinking about depression in peers. 4.3. Practical implications Based on the assumptions of AT, some theorists have suggested that encouraging people to attribute mental disorder to the medical basis of the condition will reduce stigmatizing reactions toward people with mental disorders (see Corrigan and Watson, 2004; Hinshaw and Stier, 2008). While such interventions assume that a medical cause will reduce perceptions of personal control, it overlooks environmental causes which can be perceived as low on personal control. In addition, the findings of a recent meta-analysis (Kvaale et al., 2013) indicate mixed consequences for the medicalization of mental disorders. They found that people who hold biogenetic explanations for mental disorders tend to blame affected persons less for their problems, but desire more distance from them. Therefore our research would indicate that educational interventions should seek to teach adolescents about the known causes of different disorders and, as Weiner et al. (1988) suggest, highlight the array of determinants (both genetic and environmental) of the onset of stigmatized disorders. Rather than emphasizing genetic causes for depression, interventions should be informed by the latest research on known causes. 9 Our findings indicate that when a cause is perceived as low on personal control, responsibility is not inferred, sympathy is felt, and this has a positive effect on social acceptance. Dowey et al. (2007) found that a one-day training workshop can change care staff's causal thinking about challenging behaviors in individuals with intellectual disabilities. It is possible that a brief intervention could change adolescent causal attributions about depressed behavior in peers, with the aim of reducing perceptions of personal control. However, Weiner et al. (1988) suggested that perceptions of controllability of the onset of mental-behavioral stigmas can be altered in the direction of uncontrollability. While this produces more positive emotions and behavioral reactions, it also causes a dilemma. On one hand it seems necessary for individuals to accept responsibility for their behavior (it promotes personal change and is the basis for many psychotherapies). On the other hand, altruistic actions from others are augmented by perceptions of uncontrollability (Weiner et al., 1988). A further concern is that if interventions describe disorders like depression as having uncontrollable components, it may lower the expectation of recovery (Corrigan and Watson, 2004; Weiner et al., 1988) and have negative consequences such as discouraging those close to individuals with depression from suggesting self-initiated actions towards recovery. In addition, our findings highlight the significance of gender when considering the stigma of depression during adolescence. Both the gender of the individual with depression and the gender of the peer responding to that individual emerged as significant variables in our research. Specifically we found that adolescents feel anger toward a male peer who is deemed responsible for his depression, females are more likely to socially accept a female peer with depression, and males are more likely to perceive other males as having control over the onset of depression. Thus, it may be necessary to design educational interventions that directly address the issue of gender from both perspectives. 4.4. Limitations Though use of vignettes is common in this line of research (Swords et al., 2011; Peterson et al., 1985), their ecological validity has been called into question. Research indicates that attributional responses between vignettes and real life situations differ (Lucas et al., 2009). Though some researchers have explored attitudes and reactions towards actual classmates (Juvonen, 1991) rather than hypothetical vignette characters, this produces an ethical dilemma when researching attitudes towards adolescents with depression. In addition, we used explicit self-report measures of causal attributions, peer acceptance etc. Implicit measures may be valuable for tapping into adolescents' responses, and may be more resistant to desirability (for a critical discussion of this, see Gawronski et al., 2007). In terms of gender, O'Driscoll et al. (2012) found that adolescent males hold stronger negative implicit evaluations of depression compared to their female counterparts, indicating that male adolescents are motivated to inhibit their explicit negative evaluations of depression. Regarding analysis, our study did not take into account the possibility of bidirectional relations, the analysis was restricted in line with Weiner's (1993) linkages proceeding from thinking to feeling to acting. Additionally, as models were tested using cross-sectional data, caution must be exerted in inferring causality from these findings. Finally, as this study focused specifically on responses to depression, these results are not generalizable to other mental disorders in adolescence. 10 4.5. Future research Future research should further examine gender differences in responses to adolescents with depression, and should consider applying different methods (e.g. use of implicit measures). As depression is more common in females during adolescence (Dooley et al., 2012; Nolen-Hoeksema et al., 1994; Hankin et al., 1998), it is possible that responses to females with depression are more heavily influenced by familiarity with depressive symptoms. For example, recent research on depression stigma among young people (15-25 year olds) indicated that contact with mental disorders in family or friends is linked to lower levels of stigma and lower desire for social distance (Yap et al., 2013). Future research in this area should account for adolescent familiarity with depression. Qualitative studies addressing this issue would be advantageous to provide insight into how adolescents' perceive symptoms of depression in their peers. On a practical level, future educational interventions aimed at tackling stigmatizing or negative reactions to peers displaying symptoms of depression, could apply certain aspects of AT in their design but, as aforementioned, must exert caution when doing so. 4.6. Conclusion This study furthers our understanding of how teenagers evaluate and react to the behavior of a peer with depression. Key findings indicate that peer group acceptance of an adolescent with depression is predicted by low attributions of personal control, low inferences of responsibility, and emotional reactions of sympathy/pity rather than anger/irritation. When responding to a male peer with depression, male participants perceive them as having more personal control over the causes of their behavior than female participants. When responding to a female peer with depression, female participants are more likely to socially include them than their male counterparts. The findings of this study build on our theoretical understanding of why adolescents with depression may face social exclusion from peers, and should be incorporated into interventional efforts aimed at reducing peer exclusion and stigmatization of adolescents with depression. 11 Acknowledgements We thank the adolescents who participated in this study, their parents who gave permission for their participation and the schools who provided the time and space to facilitate the collection of data. 12 References Achenbach, T. M., 1991., Integrative guide for the 1991 CBCL/4-18, YSR, and TRF profiles. Burlington, VT: University of Vermont, Department of Psychiatry. American Psychiatric Association., 1994. Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: Author. Anderson, C.A., Arnoult, L.H., 1985. Attributional style and the everyday problems in living: depression, loneliness, and shyness. Social Cognition 3, 16-35. Bollen, K.A., Long, J.S., 1993. Testing Structural Equation Models. Sage, Newbury Park, CA. Browne, M.W., Cudeck, R., 1993. Alternative ways of assessing model fit. In K.A. Bollen, J.S. Long, Testing Structural Equation Models. Sage, Newbury Park, CA. Corrigan, P., Markowitz, F.E., Watson, A., Rowan, D., Kubiak, M.A., 2003. An attribution model of public discrimination towards persons with mental illness. Journal of Health and Social Behavior 44, 162-179. Corrigan, P.W., Watson, A.C., 2004. At Issue: Stop the Stigma: Call Mental Illness a Brain Disease. Schizophrenia Bulletin 30, 477-479. Dooley, B., Fitzgerald, A., 2012. My World Survey. National Study of Youth Mental Health. Headstrong- National Centre for Youth Mental Health, Dublin. Dowey, A., Toogood, S., Hastings, R.P., Nash, S., 2007. Can brief workshop interventions change care staff understanding of challenging behaviours? Journal of Applied Research in Intellectual Disabilities 20, 52–57. Gawronski, B., LeBel. E.P., Peters, K.R., 2007. What do implicit measures tell us? Scrutinizing the validity of three common assumptions. Perspectives on Psychological Science 2, 181-193. Hankin, B.L., Abramson, L.Y., Moffitt, T.E., Silva, P.A., McGee, R., Angell, K.E., 1998. Development of depression from preadolescence to young adulthood: emerging gender differences in a 10year longitudinal study. Journal of Abnormal Psychology 107, 128-140. Hinshaw, S.P., Stier, A., 2008. Stigma as Related to Mental Disorders. Annual Review of Clinical Psychology 4, 367-393. Jones, C., Hastings, R.P., 2003. Staff reactions to self-injurious behaviours in learning disability services: attributions, emotional responses and helping. British Journal of Clinical Psychology 42, 189-203. Juvonen, J., 1991., Deviance, perceived responsibility, and negative peer reactions. Developmental Psychology 27, 672-681. Kenny, R., Dooley, B., Fitzgerald, A., 2013. Interpersonal relationships and emotional distress in adolescence. Journal of Adolescence 36, 351-360. 13 Kvaale, E.P., Gottdiener, W.H., Haslam, N., 2013. Biogenetic explanations and stigma: a metaanalytic review of associations among laypeople. Social Science & medicine, 96, 95-103. La Greca, A.M., Moore Harrison, H., 2005. Adolescent peer relations, friendships, and romantic relationships: do they predict social anxiety and depression? Journal of Clinical Child and Adolescent Psychiatry 34 , 49-61. Lewinsohn, P.M., Rohde, P., Seeley, J.R., 1998. Major depressive disorder in older adolescents: prevalence, risk factors and clinical implications. Clinical Psychology Review 18, 765–794. Link, B.G., Phelan, J.C., 2001. Conceptualizing stigma. Annual Review of Sociology 27, 363-385. Lucas, V.L., Collins, S., Langdon, P.E., 2009. The causal attributions of teaching staff towards children with intellectual disabilities: a comparison of ‘vignettes’ depicting challenging behaviour with ‘real’ incidents of challenging behaviour. Journal of Applied Research in Intellectual Disabilities 22, 1-9. MacLean, A., Hunt, K., Sweeting, H., 2012. Symptoms of mental health problems: children's and adolescents' understandings and implications for gender differences in help seeking. Children & Society 27, 161-173. Martin, J.K., Pescosolido, B.A., Tuch. S.A., 2000. Of fear and loathing: the role of 'disturbing behavior', labels, and causal attributions in shaping public attitudes toward people with mental illness. Journal of Health and Social Behavior 41, 208-223. McAuley, E., Duncan, T.E., Russell, D.W., 1992. Measuring causal attributions: the revised Causal Dimension Scale (CDSII). Personality and Social Psychology Bulletin 5, 566-573. Meyer. J.P., Mulherin. A., 1980. From attribution to helping: an analysis of the mediating effects of affect and expectancy. Journal of Personality and Social Psychology 39, 201-210. Nolen-Hoeksema, S., Girgus, J.S., 1994. The Emergence of gender differences in depression during adolescence. Psychological Bulletin 115, 424-443. O'Driscoll, C., Heary, C., Hennessy, E., McKeague, L., 2012. Explicit and implicit stigma towards peers with mental health problems in childhood and adolescence. Journal of Child Psychology and Psychiatry 53, 1054–1062. Peterson, L., Mullins, L.L., Ridley- Johnson, R., 1985. Childhood depression: peer reactions to depression and life stress. Journal of Abnormal Child Psychology 13, 597-609. Schmidt, G., Weiner, B., 1988. An attribution-affect-action theory of behaviour: replications of judgments of help-giving. Personality and Social Psychology Bulletin 14, 610-621. Sigelman, C. K., Begley, N. L., 1987. The early development of reactions to peers with controllable and uncontrollable problems. Journal of Pediatric Psychology 12, 99-115. Siperstein, G.N., 1980. Adjective Checklist (ACL) and Friendship Activity Scale (FAS): Instruments for measuring children's attitudes. University of Massachusetts, Center for Social Development and Education, Boston. 14 Steinhausen, H., Metzke, C.W., 2001. Risk, compensatory, vulnerability, and protective factors influencing mental health in adolescence. Journal of Youth and Adolescence 30, 259-280. Stice, E., Ragan, J., Randall., 2004. Prospective relations between social support and depression: differential direction of effects for parent and peer support? Journal of Abnormal Psychology 113, 155-159. Swords, L., Heary, C., Hennessy, E., 2011. Factors associated with acceptance of peers with mental health problems in childhood and adolescence. Journal of Child Psychology and Psychiatry 52, 933-941. Weiner, B., 1985. An attributional theory of achievement motivation and emotion. Psychological Review 92, 548-573. Weiner, B., 1986. An Attributional Theory of Motivation and Emotion. Springer, New York. Weiner, B., 1993. On sin versus sickness: a theory of perceived responsibility and social motivation. American Psychologist 48, 957-965. Weiner, B., 1995. Judgments of Responsibility: A Foundation for a Theory of Social Conduct. The Guilford Press, New York. Weiner, B., Graham, S., Chandler, C., 1982. Pity, anger, and guilt: an attributional analysis. Personality and Social Psychology Bulletin 8, 226-232. Weiner, B., Perry, R., Magnusson, J., 1988. An attributional analysis of reactions to stigmas. Journal of Personality and Social Psychology 55, 738-748. World Health Organisation., 1992. ICD-10 Classifications of Mental and Behavioural Disorder: Clinical Descriptions and Diagnostic Guidelines. World Health Organisation, Geneva. Yap, M.B.H., Reavley, N., Mackinnon, A.J., Jorm, A.F., 2013. Psychiatric labels and other influences on young people's stigmatizing attitudes: findings from an Australian national survey. Journal of Affective Disorders 148, 299-309. 15 Appendices Appendix A: Vignettes of male and female adolescent with symptoms of depression Male vignette Neil is the same age as you. He used to enjoy playing sports and hanging around with his friends after school. However, recently he has stopped going to training and doesn’t come out much in the evenings, saying he is too tired and spending most of his time in his room. He rarely replies to texts or signs onto Facebook chat or MSN. He often seems irritated and distracted in school. He used to get good marks but is falling behind in schoolwork and finds it hard to concentrate and pay attention in class. When his teachers asked him about this he says he can’t be bothered about schoolwork anymore and doesn’t see the point in trying to improve. His friends have noticed he doesn’t eat much at break time and has lost weight. They also feel he is not himself and it’s hard to get a laugh out of him anymore. Sometimes while talking to people his eyes water and he seems like he might cry for no reason but he says he has hay-fever to cover up how he feels. He looks very tired and doesn’t care about his appearance anymore. Neil spends a lot of time thinking about the things he cannot do and feels an overwhelming sadness that makes everything not worth bothering with. He often feels that his life is not worth living anymore. He looks back on his old life as if it belongs to someone else and, even when he is around his friends, feels very lonely. Female vignette Kate is the same age as you. She used to enjoy playing sports and hanging around with her friends after school. However, recently she has stopped going to training and doesn’t come out much in the evenings, saying she is too tired and spending most of her time in her room. She rarely replies to texts or signs onto Facebook chat or MSN. She often seems irritated and distracted in school. She used to get good marks but is falling behind in schoolwork and finds it hard to concentrate and pay attention in class. When her teachers asked her about this she says she can’t be bothered about schoolwork anymore and doesn’t see the point in trying to improve. Her friends have noticed she doesn’t eat much at break time and has lost weight. They also feel she is not herself and it’s hard to get a laugh out of her anymore. Sometimes while talking to people her eyes water and she seems like she might cry for no reason but she says she has hay-fever to cover up how she feels. She looks very tired and has stopped wearing makeup. Kate spends a lot of time thinking about the things she cannot do and feels an overwhelming sadness that makes everything not worth bothering with. She often feels that her life is not worth living anymore. She looks back on her old life as if it belongs to someone else and, even when she is around her friends, feels very lonely. 16 Table 1: Descriptive statistics for questionnaire items used in SEM model with male vignette character (n=199; model A) and female vignette character (n=202; model B) Latent Variable Measured Variable Range Model M (SD) Factor loading Personal Control y1 CDS-II item 1 1.00-9.00 A B 4.30 (2.14) 4.32 (2.12) 0.88*** 0.79*** y2 CDS-II item 2 1.00-9.00 A B 5.07 (2.41) 4.92 (2.39) 0.59*** 0.68*** y3 CDS-II item 3 1.00-9.00 A B 6.82 (2.01) 6.99 (2.17) 0.59*** 0.66*** y4 Responsibility item (no factor loading as observed variable) y5 Positive emotion item1 (pity) 1.00-6.00 A B 4.47 (1.40) 4.54 (1.50) - 1.00-6.00 A B 4.48 (1.32) 4.43 (1.42) 0.46*** 0.33* y6 Positive emotion item 2 (sympathy) 1.00-6.00 A B 4.74 (1.12) 4.44 (1.46) 0.61*** 0.80* y7 Negative emotion item 1 (anger) 1.00-6.00 A B 2.55 (1.39) 2.74 (1.43) 0.58* - y8 Negative emotion item 2 (irritation) 1.00-6.00 A B 3.16 (1.51) 3.05 (1.60) 0.50*** - y9 FAS Question 1 1.00-4.00 A B 2.73 (0.71) 2.71 (0.79) 0.48*** 0.69*** y10 FAS Question 2 1.00-4.00 A B 3.59 (0.66) 3.61 (0.66) 0.39*** 0.40*** y11 FAS Question 3 1.00-4.00 A B 3.40 (0.63) 3.45 (0.67) 0.55*** 0.58*** y12 FAS Question 4 1.00-4.00 A B 2.36 (0.76) 2.46 (0.89) 0.51*** 0.65*** y13 FAS Question 5 1.00-4.00 A B 2.94 (0.73) 2.92 (0.80) 0.52*** 0.63*** y14 FAS Question 6 1.00-4.00 A B 3.79 (0.48) 3.81 (0.45) 0.53*** 0.43*** y15 FAS Question 7 1.00-4.00 A B 3.33 (0.86) 3.49(0.76) 0.45*** 0.42*** y16 FAS Question 8 1.00-4.00 A B 2.84(0.79) 2.74 (0.85) 0.66*** 0.70*** y17 FAS Question 9 1.00-4.00 A B 2.51(0.87) 2.51(0.94) 0.31*** 0.53*** y18 FAS Question 10 1.00-4.00 A B 3.39(0.61) 3.38(0.71) 0.46*** 0.40*** y19 FAS Question 11 1.00-4.00 A B 3.44(0.67) 3.57(0.65) 0.35*** 0.52*** y20 FAS Question 12 1.00-4.00 A B 3.36(0.67) 3.42(0.74) 0.52*** 0.68*** y21 FAS Question 13 1.00-4.00 A B 2.78(0.82) 2.56(0.89) 0.63*** 0.62*** Responsibility Positive emotions Negative emotions Behavioural Intentions *p < 0.05. **p < 0.01. *** p < 0.001. (ns) = not significant 17 y9 Participant Gender* y5 y10 y6 y11 y1 y2 y12 Positive Emotions y3 y13 y14 Personal Control Peer Acceptance Responsibility (y4) y15 y16 Negative Emotions y17 y18 y19 y7 y8 y20 y21 Figure 1: Path diagrams of the direct and indirect relationships between factors predicting adolescents' behavioural intentions towards a peer with depression. Latent variables are represented as ovals, and measured items/observed variables (y1-y21) are represented as rectangles. The measurement error of each item has been omitted to lessen complexity. Arrows connecting the latent variables and the items that comprise them are factor loadings. Single headed arrows between variables are regression pathways. *Participant Gender was coded 1 for male participants and 2 for female participants. Therefore positive values between participant gender and another variable, indicates a relationship with female gender and negative values indicate a relationship with male gender. 18 0.17 Participant Gender 0.13 Positive Emotions -0.03 -0.20* 0.50** -0.28* Personal Personal Control Control Peer Acceptance Responsibility 0.40*** 0.31* 0.17 Negative Emotions 0.02 Figure 2: Standardised solutions for model A; male vignette character (n=199). *=p < 0.05, **=p < 0.01, ***=p < 0.001 19 0.20* Participant Gender 0.22 Positive Emotions 0.03 0.43** -0.09 -0.23* Personal Personal Control Control Peer Acceptance Responsibility 0.49*** 0.09 0.02 Negative Emotions 0.01 Figure 3: Standardised solutions for model B; female vignette character (n=202). *=p < 0.05, **=p < 0.01, ***=p < 0.001 20