Clinical Details Form
advertisement

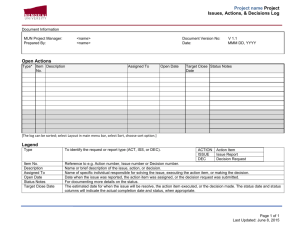
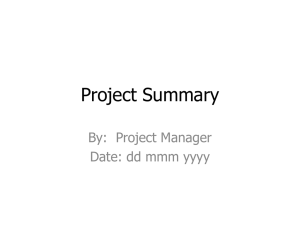
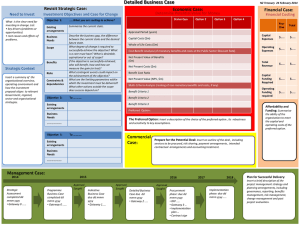
2 Screening number Initials Day 0 Month 1 Year DEMOGRAPHIC DETAILS A Age If not aged between 16 and 45 patient is ineligible White Mixed – white & Asian Black Caribbean Mixed – white & black Caribbean Asian Bangladeshi Asian - Indian Mixed – other Mixed – white & black African Asian - other Asian Pakistani Chinese Black African Black - other Other ethnic group Not stated If other ethnic group please specify Do you currently smoke? Have you ever smoked? Yes No How many per day? Yes No If yes, Date stopped? _DD / MMM / YYYY CLINICAL OBSERVATIONS Height (cm) Weight (kgs) BMI BP (mm/Hg) RELEVANT MEDICAL HISTORY (please include dates) Medical History Date _DD / MMM / YYYY _DD / MMM / YYYY _DD / MMM / YYYY _DD / MMM / YYYY _DD / MMM / YYYY _DD / MMM / YYYY _DD / MMM / YYYY _DD / MMM / YYYY CONCOMITANT MEDICATIONS Current Medications (regular over last 3 months) Name Dose Frequency Yes No Start Date Stop Date _DD / MMM / YYYY _DD / MMM / YYYY _DD / MMM / YYYY _DD / MMM / YYYY _DD / MMM / YYYY _DD / MMM / YYYY _DD / MMM / YYYY _DD / MMM / YYYY _DD / MMM / YYYY _DD / MMM / YYYY _DD / MMM / YYYY _DD / MMM / YYYY Page 1 of 3 PRE-EMPT study Clinical details screening CRF Version 1.0 13th March 2014 13/NS/0103 Indication 2 Screening number Initials Day Month 0 1 Year CONCOMITANT MEDICATIONS GYNAECOLOGICAL HISTORY Parity + Date of last menstrual cycle Comments _DD / MMM / 2 0 YY_ Previous treatments (prior to current laparoscopy) (give relevant advice according to treatment allocated) Please Reason for treatment CPP (chronic pelvic pain) LNG-IUS Yes Post op prevention No Contraception Heavy menstrual bleeding CPP (chronic pelvic pain) DMPA Yes Post op prevention No Contraception Heavy menstrual bleeding CPP (chronic pelvic pain) COCP Yes Post op prevention No Contraception Heavy menstrual bleeding If other reason: Previous GnRha Yes No Which type? Previous HRT Yes No Which type? Previous laparoscopy Yes No Date _DD / MMM / 2 0 YY_ Previous laparoscopy Yes No Date _DD / MMM / 2 0 YY_ Previous laparoscopy Yes No Date _DD / MMM / 2 0 YY_ Pregnancy test Yes No Positive Negative Date Chlamydia test result Yes No Positive Negative Date _DD / MMM / 2 0 YY_ _DD / MMM / 2 0 YY_ If pregnancy positive patient is ineligible. If Chlamydia positive – do not insert IUS until treated SCREENING ELIGIBILITY Patient fulfils screening criteria? Yes No Consent form signed? Yes No Baseline questionnaire completed and signed? Yes No CONTINUE WITH FORM AT TIME OF SURGERY Page 2 of 3 PRE-EMPT study Clinical details screening CRF Version 1.0 13th March 2014 13/NS/0103 2 Screening number Initials Day 0 Month 1 Year SURGERY DETAILS Name of surgeon Date of surgery _DD / MMM / 2 0 YY_ Type of Surgery (please tick) Diagnostic/Therapeutic (2 stage) See & Treat Extent of excision (Opinion of Surgeon) Complete Incomplete i (minimal) ii (mild) Were digital images of endometrial lesions captured during Laparoscopy Yes No Ovarian Endometriosis present Yes No AFS Stage of Endometriosis iii (moderate) iv (severe) Please enter 4 digit Randomisation number SIGNATURE OF CLINICIAN _DD / MMM / 2 0 YY_ Clinician’s Signature Date COMPLIANCE WITH TREATMENT ALLOCATION Day of menstrual cycle (give relevant advice according to treatment allocated) TREATMENT COMPLICATIONS (If ‘yes’, please complete an AE form to determine if the complication is deemed Treatment Please How was this administered / prescribed? Please Reason serious toallocated report as an SAE) During Surgery TES Before discharge SIGNATURE LNG-IUS Referred to GP/Sexual Health Clinic Failure to fit Declined (please state reason) During Surgery Before discharge DMPA Referred to GP/Sexual Health Clinic Failure to administer Declined (please state reason) First cycle of tablets given to patient Prescription dispensed in hospital COCP Referred to GP/Sexual Health Clinic Declined (please state reason) SURGICAL COMPLICATIONS (If ‘yes’, please complete an AE form to determine if the complication is deemed serious to report as an SAE) Any complications Yes No If ‘yes’ please select from list below Vaso-vagal episode Cervical trauma Uterine perforation Haemorrhage If Other: specify SIGNATURE Form completed by (please print) Signed Date form completed _DD / MMM / YYYY Page 3 of 3 PRE-EMPT study Clinical details screening CRF Version 1.0 13th March 2014 13/NS/0103 2 Screening number Initials Day Month 0 1 Year Page 4 of 3 PRE-EMPT study Clinical details screening CRF Version 1.0 13th March 2014 13/NS/0103