- D-Scholarship@Pitt
advertisement

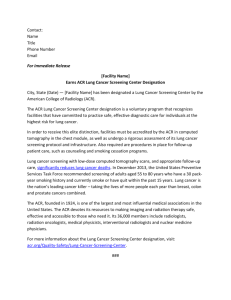
USING LOW DOSE COMPUTED TOMOGRAPHY IN LUNG CANCER SCREENING by Hazim Ogorban M.B.Ch.B, Tripoli University, Libya, 2003 Submitted to the Graduate Faculty of the Multidisciplinary MPH Program Graduate School of Public Health in partial fulfillment of the requirements for the degree of Master of Public Health University of Pittsburgh 2013 UNIVERSITY OF PITTSBURGH GRADUATE SCHOOL OF PUBLIC HEALTH This essay is submitted by Hazim Ogorban December , 2013 Essay Advisor: David Finegold, MD Director, Multidisciplinary MPH Program Professor, Department of Human Genetics Graduate School of Public Health University of Pittsburgh ______________________________________ Essay Reader: Joel Weissfeld, MD, MPH Associate Professor Department of Epidemiology Graduate School of Public Health University of Pittsburgh ______________________________________ Essay Reader: Thomas Songer , PhD Assistant Professor Department of Epidemiology Graduate School of Public Health University of Pittsburgh ______________________________________ ii Copyright © by Hazim Ogorban 2013 iii David Finegold, MD USING LOW DOSE COMPUTED TOMOGRAPHY IN LUNG CANCER SCREENING Hazim Ogorban, MPH University of Pittsburgh, 2013 Abstract More people, in the United States and worldwide, die from lung cancer than breast, colon, or any other type of cancer. Although, efforts to reduce tobacco smoking have decreased incidence rates in the U.S, lung cancer remains a public health issue that needs an effective intervention. Results from the National Lung Screening Trial (NLST) demonstrate that screening high risk individuals with low dose computed tomography (LDCT) can have a significant impact on mortality rates of lung cancer. However, implementing a lung screening program in real world practice could be a challenging task. Therefore, medical and public health institutions should be prepared with necessary resources, adhere to a standard practice for lung cancer screening, decrease health care disparities, and enhance public participation. This review presents some key statistics for lung cancer in the U.S, an overview of lung cancer screening studies and the impact of radiological settings and lung nodule management protocols in detecting cancer lesions, and discusses issues related to implementation of a national screening program. iv TABLE OF CONTENTS 1.0 2.0 INTRODUCTION............................................................................................................... 1 1.1 BACKGROUND ..................................................................................................... 1 1.2 LUNG CANCER STATISTICS IN THE U.S ..................................................... 2 1.2.1 Incidence .......................................................................................................... 2 1.2.2 Mortality .......................................................................................................... 3 1.2.3 Survival Rates................................................................................................. 5 LITRETURE REVIEW…………………………………..…………………………………………… 5 2.1 OVERVIEW OF LUNG CANCER SCREENING STUDIES ............................. 5 2.1.1 The National Lung Screening Trial (NLST)……………………………………….. 5 2.1.2 The Dutch-Belgian Randomized Lung Cancer Screening Trial …………...... 6 2.2.3 Other randomized clinical trials and observational studies………………….…7 2.2 IMPLEMENTATION…………………………………………………………………………8 2.2.1 Selection criteria…………………………………………………………………………….10 2.2.2 A multidisciplinary health care team …………………………………………………11 2.2.3 Lung nodule diagnosis and management ………………………………………..…..12 2.2.4 CT settings and quality assurance …………………………………………………….13 2.2.5 False positives and invasive procedures ……………………………………………..14 v 3.0 DISCUSSION.....................................................................................................................15 BIBLIOGRAPHY ....................................................................................................................... 18 vi LIST OF FIGURES Figure 1: Age-adjusted incidence rates of lung & bronchus cancer in the United States.............3 Figure 2: Age-adjusted mortality rates of lung & bronchus cancer in the United States…………4 Figure 3: Interactions among different health institutions and stakeholders in lung cancer screening……………………………………………………………………………………...………………..…...11 1.0 INTRODUCTION 1.1 BACKGROUND In the United States, lung cancer is the leading cause of cancer death among men and women. In 2010, 201,144 individuals were diagnosed and 158,248 died from lung cancer [1]. According to the American Cancer society, there will be an estimated 228,190 new cases and 159,480 deaths from lung cancer in 2013 [2]. When compared to breast and colorectal cancers, death rates from lung cancer exceeds the death rate of both previous cancers combined. For breast cancer, the estimated new cases and death rates in 2013 are 234,580 cases and 40,030 deaths, respectively. And colorectal cancer is estimated to account for 142,820 new cases and 50,830 deaths in the same year [3]. The latest U.S available data indicate that lung cancer is accountable for approximately 14% of all newly diagnosed cancer cases. Most of these new patients (31.4%) are between 65 and 74 years old, and the median age of death due to lung cancer is 72 years of age [4]. The 5-year survival rate for lung cancer is 17%, in breast cancer the rate is 90%, and 65% for colon cancer [3]. Despite the poor prognosis and survival rates for lung cancer, detecting an early stage tumor has a better chance to be treated than late stage disease [2]. The effectiveness of various approaches for detecting and treating early lung cancer has been a major public health interest for many years [5]. In 2011, results from the National Lung Screening Trial (NLST) showed a 20% decrease in lung cancer mortality in individuals screened with a low dose CT (LDCT) compared to a control group receiving regular chest x-rays. The study also reported that, 320 individuals needed to be screened in order to prevent 1 person from lung cancer death [6]. Whether a national lung screening program follows the NLST or a similar protocol, the major concern, will be effectiveness in practice, associated with lowered lung cancer mortality, improved cancer outcomes, and minimum harm. 1 1.2 LUNG CANCER STATISTICS IN THE UNITED STATES 1.2.1 Incidence Data from the National Cancer Institute (Surveillance, Epidemiology, and End Results Program) show that between 2006 and 2010, age-adjusted U.S lung cancer incidence rate for all ages, all races, male and female was 61.4 per 100,000 persons. Rates were 356 and 18.6 per 100,000 for person’s ≥ 65 and ≤ 65 years, respectively. Males aged 65 and over had an incidence rate of 443.3 per 100,000, while the rate in female was 294.6 per 100,000. In general, the black (male and female) race had a higher incidence rate than the white race. However, black males had higher incidence rates than white males and white females had higher rates than black females [7]. Age specific incidence rates for both sexes between 2006 and 2010 were below 200 per 100,000 for both age groups 55-59 years and the age group 60-64 years. The 65-69 years age group and the 70-74 years age group had an incidence rate of 267.4 per 100,000 and 359 per 100,000 individuals, respectively. The rate was above 400 for both age groups 75-79 years and 80-84 years [7]. Figure (1) shows the U.S age-adjusted (2000 U.S standard population) lung & bronchus cancer incidence rates by gender, race, and age group from 1973 to 2010, generated from the Surveillance, Epidemiology, and End Results Program, using SEER*Stat software version 8.1.2 [8]. 2 Incidence 400 350 Rate per 100,000 300 65+ years 250 55-64 years 200 Male Black 150 White 100 Female Under 55 years 50 2009 2007 2005 2003 2001 1999 1997 1995 1993 1991 1989 1987 1985 1983 1981 1979 1977 1975 1973 0 Year of diagnosis Figure (1) Age-adjusted incidence rates of lung & bronchus cancer in the United States based on Surveillance, Epidemiology, and End Results Program data released in April 2013. 1.2.2 Mortality The age adjusted U.S lung cancer death rate between 2006 and 2010 for all ages, all genders, and all races was 49.5 per 100,000 persons. The mortality rate for those under 65 years of age was 14 per 100,000 and the rate was 294.3 per 100,000 for people 65 years and older. Males had higher rates than females and black males aged 65 and older had the highest death rates. Otherwise there was a slight difference between white (both genders) and black (both genders) races. The age specific mortality rate between 2006 and 2010 for both male and female, all races was 120 3 per 100,000 for individuals between 60 and 64 years of age, 200 per 100,000 for the age group 65-69 years, 280 per 100,000 for those between 70 and 74 years, and above 300 per 100,000 for all the other older age groups [7]. Figure (2) shows the U.S age-adjusted (2000 U.S standard population) lung & bronchus cancer mortality rates by gender, race, and age group from 1969 to 2010, generated from the Surveillance, Epidemiology, and End Results Program, using SEER*Stat software version 8.1.2 [9]. Mortality 350 Rate per 100,000 300 250 65 + years 200 55-64 years Male 150 Black 100 White 50 Female Under 55 years 1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 0 year of death Figure (2) Age-adjusted mortality rates of lung & bronchus cancer in the United States based on Surveillance, Epidemiology, and End Results Program data released in April 2013. 4 1.2.3 Survival Rates The five-year survival rate for lung cancer cases diagnosed at an early stage (localized within the lung) is 53.3%. For regional lung cancer (cancer spread to nearby lymph nodes) the rate is 26 % and the five-year survival rate for late stage disease (cancer spread to other organs) is 3.9%. However, only 15% of malignant lung cancer cases are discovered at an early stage and 57% diagnosed at a late stage [4]. The five-year survival rate for lung cancer between 1975 and 1977 was 12.2% and between 2003 and 2009 the rate was 17.5%. This slight improvement in survival is much less than that observed for other cancers. For example, the five-year survival rate of breast cancer between 1975 and 1977 was 74.8% and the rate increased to 90.3% between 2003 and 2009. For colon cancer the rates improved from 50.6% to 65.4% between the years 19751977 and 2003-2009. Likewise, prostate cancer’s five-year survival rate increased from 67.8% to 99.7% [7]. 2.0 LITERATURE REVIEW 2.1 OVERVIEW OF LUNG CANCER SCREENING STUDIES 2.1.1 The National Lung Screening Trial (NLST) The NLST is the largest randomized clinical trial (RCT) for lung cancer screening. 53,454 individuals were enrolled in the study, 26,722 of them were randomly assigned to a low dose CT (LDCT) group comparing them to another group that received chest-x-ray screening. Annual screening for 3 years was conducted with a 94% follow up rate in the first year and a 92% in the second year [6]. Screening was performed in multiple centers, with different brands of imaging 5 equipment. The main characteristics assessed were nodule diameter. A non-calcified nodule equal or more than 4mm in diameter was considered a positive result. All the CT scanners used satisfied NLST protocol requirements, including detector collimation of 2.5 mm or less, a reconstruction slice width 1-3.2 mm, and a scanning time of less than 25 seconds. The NLST showed a 20% decrease in lung cancer mortality [6, 10]. 2.1.2 The Dutch-Belgian Randomized Lung Cancer Screening Trial (NELSON) The NELSON study is the largest RCT for LDCT screening in Europe, which compared CT screening with usual care (no screening). A total of 15,822 participants, 7557 of them were screened by LDCT in 3 rounds, year 1, 2 and 4 and followed for 10 years since randomization. Screening was conducted in 4 sites; with 16-detector CT Siemens and Philips scanners. Scanning was performed in a spiral mode, 1 mm slice thickness, and a 0.7 mm reconstruction interval. Nodule diameter and volume were assessed and volumetric software was used to help in diagnosis. Images were read by 2 and sometimes 3 radiologists with experience in reading thoracic CT scans [11, 12]. A test was positive if a non-calcified nodule was more than 500 mm3 or had a 25% increase in volume (volume doubling time) in less than 400 days, and intermediate if it was 50-500 mm3 or had a volume doubling time (VDT) from 400-600 days. In the LDCT group, 2.6% of scans were positive at baseline and 1.8% at the second screening round. Participants who had an intermediate test at baseline and had a positive result in a 3 month follow-up CT scan, were counted in the 2.6%. The study had a 95% adherence at baseline and 92% at the second round. Lung cancer detection rates were 0.9% at baseline and 0.5% at the second round respectively [11, 12]. 6 2.2.3 Other randomized clinical trials and observational studies The Pittsburgh Lung Screening Study (PLuSS): This was an observational study that enrolled 3642 participants. Subjects received an annual lung CT scan and were followed for 3 years. Radiologists measured nodule diameter as the main characteristic to classify lung nodules. After 3 years from the first CT scan performed, the study identified 80 (2.2%) cases of primary lung cancer; one-half of those patients had stage I nonsmall cell cancer. Although, the study showed high rates of early stage cancer detection, there was a large number of people, 36 individuals (1% of the total screened), that underwent invasive procedures, such as thoracotomy, video assisted thoracoscopic surgery, mediastinoscopy, and median sternotomy, which later on were found to have benign lesions [13]. In 2011, the PLuSS team reported that they accumulated more than 150 lung cancer diagnosis in subjects who enrolled in the study [14]. The Danish Randomized Lung cancer CT Screening Trial (DLCST): The DLCST included 4014 individuals randomized to annual screening or no screening (usual care) for 5 rounds [15]. The study was performed in one center using Philips CT scans, 1-3 mm slice thickness, and 1-1.5 mm reconstruction interval. Images were assessed according to diameter and volume by 2 board certified radiologists and used the same volumetric software used in the NELSON study [10, 12& 15]. In the screening group 69 lung cancers were diagnosed throughout the study compared with 24 in the control group, which was statistically significant (P <0.001), with an overall cancer detection rate of 0.7% [16]. 7 The DANTE & ITALUNG studies: A RCT conducted in Milan, Italy, the DANTE (Detection and Screening of Early Lung Cancer by Novel Imaging Technology and Molecular Essays) trial enrolled males only aged 60 to 75 years old. 1276 subjects received an annual LDCT for 5 years and 1196 in the control group had annual medical examinations. Screening was performed in 3 sites with a Philips scanner, 5 mm thickness, 3 mm reconstruction interval, and nodule diameter was the main characteristic assessed [12, 17]. Another study conducted in Italy, the Italian Lung study (ITALUNG), is a RCT that included 1613 in the LDCT group, 1593 in the control group (no screening), and 4 annual screening rounds. The trial had 3 screening sites, using Siemens and General Electric CT scans, with slice thickness of 1-3 mm, and a reconstruction interval 1-1.5 mm [12, 18]. Two board certified radiologists with 5 or more years of experience read each CT image independently, assessing nodule diameter but not volume plus other characteristics. The study results after baseline screening show that 30.3% of individuals in the screened group had positive results. The positive results decreased during the other screening rounds by almost 50%, but still higher than most RCT conducted during that time [12, 18]. This high rate of positive results usually leads to more follow up images, invasive procedures, and more false positive cases. 2.2 Implementation Lung cancer screening trials conducted in the USA and Europe show different results, regarding cancer detection rates, reduction in mortality rates, and number of false positive results. While the NLST study demonstrated a significant decrease in lung cancer mortality and all-cause mortality, it also had a high rate of false positive and a positive predictive value < 4% [6, 19]. Studies such as the NELSON study, the second largest clinical trial after the NLST, had a higher 8 positive predictive value, 35.7% at baseline and 42.4% at the first round of screening (one year after randomization) [19]. The final results from the NELSON trial are expected in 2016, which will be very important for the future of lung cancer screening, especially in European countries. Many studies showed no difference in lung cancer mortality rates between the LDCT group and the control group, most likely due to small number of participants compared to the NLST and the NELSON studies. Therefore, it will be extremely important to follow a highly structured system similar if not better than that of the NLST study, to achieve a successful LDCT screening program in the US or any other country [20]. Some of the challenges that can face LDCT screening implementation in any regional or national health care system are: 1. Selection criteria for individuals screened. 2. Presence of a multidisciplinary health care team at screening centers. 3. Forming an efficient protocol for lung nodule diagnosis and management. 4. Unifying CT settings and quality assurance in multiple screening centers. 5. Reducing false positives and minimizing invasive procedures. 2.2.1 Selection criteria To increase benefit and decrease harm from LDCT screening, the targeted population should contain high risk individuals. The NLST study criteria used to identify those eligible for screening included, age (55 to 74 years), a history of 30 pack-years of smoking in current smokers and former smokers who stopped smoking in the last 15 years [6]. Tammemagi et al. used a modified model of the Prostate, Lung, Colorectal, and Ovarian (PLCO) cancer screening trial and re-examined the selection criteria of the NLST study. An estimated 12 deaths due to lung cancer would have been avoided if the modified PLCO (M2012) risk prediction model was 9 used [21]. Proving that sensitivity for lung cancer detection can be improved using a more complex risk model. Predictors used in this model are age, level of education, body mass index (BMI), chronic obstructive pulmonary disease (COPD), family history of lung cancer, smoking status, duration of smoking, smoking quit time, and smoking intensity [21, 22]. 2.2.2 A multidisciplinary health care team Developing a lung cancer screening program, needs a well-established infrastructure and a team of experts in different medical fields. More than one hospital and health care institute are expected to work together using a standardized protocol in managing pulmonary nodules and lung cancer disease [19]. The International Association for the Study of Lung Cancer (IASLC) recommends that a multidisciplinary team should be involved in LDCT screening, and medical centers should have the capability to provide the appropriate imaging procedures and the equipment needed in minimal and invasive procedures, such as video-assisted thorascopic surgery, which has lower morbidity and mortality, and leads to less hospital stay than open surgeries [22, 23]. Primary care physicians and physician assistants will have a major role in selecting eligible patients and managing lung nodules. For this reason, it is very important that they are educated and regularly updated with the latest evidence based information regarding lung cancer screening, its benefit, and the risks involved. They should also be provided with all the necessary resources [19]. Most likely, there will be a huge number of people living in rural areas and underserved communities, who will face difficulties in showing up for screening and follow up sessions. Therefore, large medical centers with the proper surgical and technical facilities should cooperate with family practices and health care professionals working in those areas, to ensure 10 that most patients, if not all, receive sufficient care, regular follow up, and required treatment when needed. Figure (3) illustrates how institutions and stakeholders might integrate with one another in a lung cancer screening program. Primary Health Care Centers High risk individuals Specialized Medical Institutions General population CT scan screening centers Individuals needing follow up Invasive procedures and treatment centers Public health and research institutions Figure (3) Interactions among different health institutions and stakeholders in lung cancer screening. 11 2.2.3 Lung nodule diagnosis and management Some of the main characteristics used to diagnose and classify pulmonary nodules are, nodule size, location, morphology, calcification and anatomic position [6, 10-13]. Probably the most important predictor of malignancy is the size of a nodule [24]. Many randomized clinical trials used nodule diameter (2 dimensions) to assess size. Other studies, such as the NELSON trial, used volumetric software to measure nodule volume (3 dimensions). Nodules between 50500mm3 were classified as intermediate and those more than 500mm3 were positive. Intermediate results were followed after 3 months by another CT scan. Nodules that had a volume doubling time (VDT) < 400 days were suspicious for malignancy and required additional diagnostic workup [11]. In the NLST study, a non-calcified nodule more than 4mm in size was considered positive [6]. When using a 2 dimensional diameter measurement protocol, the maximum diameter of irregular shaped nodules is used to calculate their size. This can lead to overestimating the true size of a nodule and cause more false positive cases [22]. Results from Heuvelmans et al. show that, during follow-up of suspicious nodules, all the fast growing malignant tumors had a VDT equal to 232 days or less. If this VDT is used to follow and manage lung nodules it could decrease false positive referrals [25]. 3 dimension (3D) volumetric measurements evaluate the whole structure of a lung nodule. For this reason, they can give more accurate results than 2 dimension (2D) measurements [22]. The decision to use a 3D software analysis, a 2D measurement protocol, or even both in lung cancer screening programs will definitely have a crucial role in diagnosing and managing pulmonary nodules and lung cancer mortality rates in the future. 12 A study that evaluated volume doubling times in 63 non-small cell lung cancers from the Pittsburg Lung Screening Study (PLuSS), compared cancers that were visible as suspicious nodules at baseline screening with those that were discovered during follow up. Some of the main results from this study are; (1) the slow growing cancers (doubling time > 365 days) were mostly adenocarcinoma/bronchi alveolar carcinoma type of lung cancer (86.7%), while the fast growing ones (doubling times < 183 days) were mainly squamous cell lung cancer (60%); (2) two-thirds of the cancers that were visible as nodules at baseline rounds had a slow doubling time and only 10% of cancers that were first visible during a follow up CT scan had a slow doubling time. These findings are useful in managing lung nodules during follow up sessions [14]. 2.2.4 CT settings and quality assurance Conducting a large screening program that involves many medical centers, a large number of technicians, and multiple imaging procedures will probably have some degree of technical problems and errors. Therefore, it will be extremely important to constantly monitor the screening process from the beginning and detect any imaging defects to ensure high quality results and minimize radiation exposure [26]. Screening in the NLST was performed in 10 centers using different CT brands [6, 26]. Gierada et al. conducted a study to assess the effect of implementing an imaging quality assurance program on CT image quality of the NLST study. The study identified low rates of quality defects, indicating that applying a quality assurance program in large multicenter trials can reduce technical errors [26]. Results from a study that examined the effect of using different CT slice thicknesses (1.25mm, 2.5mm & 5mm) and 2 different software packages on lung volume measurement show that, 13 small lung nodules (3-10mm) were more likely to have different volume measurements than large nodules (>15mm) on both software systems when different CT slice thicknesses were used. The study also mentions that smaller nodules are better analyzed with thinner (1.25mm) CT section thickness. And different volume measurements were observed for all nodules (small and large) when different software packages were used at a 2.5 mm section thickness. Therefore, it is best to use the same type of software and CT settings when following patients with a history of a suspicious lung nodule [27]. Assessing nodule size by measuring its volume and VDT is demonstrated to be a useful diagnostic tool to differentiate between benign and suspicious lung nodules [28, 29]. However, accuracy of volumetric measurement depends on many factors, such as CT settings, type of software used, radiologists reading the image, and nodule characteristics [28-30]. Wang et al. evaluated the effect of low dose CT reconstruction settings on volumetric measurement. Their study found that using a 1mm section thickness with soft kernel reconstruction settings was superior to a 2mm section thickness in volume measurement repeatability. To avoid incorrect assessment of VDT when following a lung nodule over time, the authors recommend using the same CT reconstruction settings [28]. 2.2.5 False positives and invasive procedures Bach at al. conducted a systematic review on the benefits and harms of CT screening for lung cancer. The review reported that nearly 20% of individuals enrolled in 8 randomized control trials and 13 cohort studies had a positive result in each screening round, ranging from 3% to 30% in RCTs. Most of these positive results were benign, but led to further workup and invasive procedures [31]. In the NLST study, 27% of individuals in the LDCT group at baseline had a 14 positive result with a false positive rate of 96% and after 3 screening rounds 40% of subjects had a suspicious CT scan finding [32]. The positron emission tomography (PET) was needed in 5.5% of total individuals screened in the NLST. While invasive procedures, such as needle biopsy and bronchoscopy were conducted in 1.2% of individuals who were found to have benign lesions, in both the NLST and the NELSON study. Rates of invasive surgical procedures were 0.7% in the NLST and 0.6% in NELSON [31]. However, according to the results from the NLST study, the rate of major complications due to invasive procedures were only 0.06% in patients who had a false positive result and 11.2% in those diagnosed with lung cancer [6]. In 2011, Nair et al published an article in the European Society of Radiology, mentioning that the rate of invasive procedures practiced during nodule management in lung screening studies ranged from 0.8% to 7.5% [10]. 3.0 DISCUSSION There is no doubt that lung cancer is a major public health problem [1-4]. And the association between tobacco smoking and lung cancer is well known. The purpose of this review was to examine the latest evidence based practices and CT settings in lung cancer screening, and how they might impact the future of this devastating disease. Since the release of the NLST results, a number of recommendations and guidelines have been established for lung cancer screening, such as the American Society of Clinical Oncology guidelines [31], the American Thoracic Society [33], and the American Association for Thoracic Surgery recommendations [34]. In 2004, lung cancer screening was graded I (insufficient evidence to make recommendation) by the U.S Preventive Services Task Force (USPSTF), because there was insufficient evidence that screening by LDCT, chest x-ray or sputum cytology can decrease death rates [35]. Recently, the USPSTF released another statement recommending annual screening with LDCT for high risk 15 individuals. Lung screening was graded B, meaning that there is moderate certainty that the net benefit is moderate or substantial [36]. To enhance the effectiveness of LDCT screening in our communities, more efforts are needed to increase public participation, by reducing health disparities and improving the quality of health care services in underserved areas. Taplin et al. conducted a retrospective study to examine the causes of late stage breast cancer diagnosis. Results from the study showed that women with low income or less education had lower rates of screening and follow-up and were more likely to have a diagnosis of late stage breast cancer than women with higher socioeconomic status [37]. Another study by Coughlin et al. indicates that women from ethnic minority groups, living in poor areas, or had a lower number of office-based clinicians in their regions had higher odds of being diagnosed with late stage breast cancer [38]. Educational programs that engage community members in raising awareness of benefits and harms of cancer screening have been proven to increase public participation and decrease health care disparities [39]. Following an evidence based protocol in screening is also an important factor that determines the type and quality of the health care delivered. Many studies have shown that a substantial number of primary care physicians don’t always follow the recommended screening guidelines [40-42]. Implementing the National Prevention Strategy recommendations of the National Prevention Council can ensure a high quality, equitable, and successful screening program. These recommendations are based on four strategic directions: healthy and safe community environments, empowered people, clinical and community preventive services, and elimination of health disparities [43, 44]. 16 In conclusion, the use of low dose computed tomography in lung cancer screening is a promising public health intervention, which can have a huge impact on our communities. To establish a nation-wide screening program many efforts are needed in different community and clinical settings. First, public health professionals, researchers, and other stakeholders should pay more attention to health disparities and educate the public about lung cancer screening; and second, health care providers and medical institutions need to recognize the importance of standardized imaging settings and lung nodule management protocols during their practice. A safe and high quality screening program will help early detection of lung cancer, save more lives, and improve the health and wellbeing of people. 17 BIBLIOGRAPHY 1. Centers of Disease Control and Prevention (CDC). Lung Cancer Statistics. Retrieved from: http://www.cdc.gov/cancer/lung/statistics/ 2. American Cancer society. What are the key statistics about lung cancer? Retrieved from: http://www.cancer.org/cancer/lungcancer-non-smallcell/detailedguide/non-small-celllung-cancer-key-statistics 3. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin 2012;62:1029. 4. SEER Cancer Statistics Factsheets: Lung and Bronchus Cancer. National Cancer Institute. Bethesda, MD, http://seer.cancer.gov/statfacts/html/lungb.html 5. American Lung association. Providing Guidance on Lung Cancer Screening To Patients and Physicians. (2012). Retrieved from: http://www.lung.org/lung-disease/lungcancer/lung-cancer-screening-guidelines/lung-cancer-screening.pdf 6. Aberle DR, Adams AM, Berg CD, et al; National Lung Screening Trial Research Team. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med. 2011;365(5):395-409. 7. Howlader N, Noone AM, Krapcho M, Garshell J, Neyman N, Altekruse SF, Kosary CL, Yu M, Ruhl J, Tatalovich Z, Cho H, Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA (eds). SEER Cancer Statistics Review, 1975-2010, National Cancer Institute. Bethesda, MD, http://seer.cancer.gov/csr/1975_2010/, based on November 2012 SEER data submission, posted to the SEER web site, April 2013. 8. Surveillance, Epidemiology, and End Results (SEER) Program (www.seer.cancer.gov) SEER*Stat Database: Incidence - SEER 9 Regs Research Data, Nov 2012 Sub (19732010) <Katrina/Rita Population Adjustment> - Linked To County Attributes - Total U.S., 1969-2011 Counties, National Cancer Institute, DCCPS, Surveillance Research Program, Surveillance Systems Branch, released April 2013, based on the November 2012 submission 9. Surveillance, Epidemiology, and End Results (SEER) Program (www.seer.cancer.gov) SEER*Stat Database: Mortality - All COD, Aggregated With State, Total U.S. (19692010) <Katrina/Rita Population Adjustment>, National Cancer Institute, DCCPS, Surveillance Research Program, Surveillance Systems Branch, released April 2013. Underlying mortality data provided by NCHS (www.cdc.gov/nchs) 10. Nair A, Hansell DM. European and North american lung cancer screening experince and limitations for pulmonary nodule management. Eur radiol (2011) 21;2445-2454. 18 11. van Klaveren RJ, Oudkerk M, Prokop M, Scholten ET, Nackaerts K, Vernhout R, van Iersel CA, van den Bergh KA, van’t WS, van der Aalst C, Thunnissen E, Xu DM, Wang Y, Zhao Y, et al (2009) Management of lung nodules detected by volume CT scanning.N Engl J Med 361:2221–2229 12. Field JK, van Klaveren R, Pedersen JH, Pastorino U, Paci E, Becker N, Infante M, Oudkerk M, de Koning HJ; on behalf of the European Randomized Screening Trial Group. (2013) European randomized lung cancer screening trials: Post NLST. J Surg Oncol. 2013;108:280-286. 13. Wilson DO, Weissfeld JL, Fuhrman CR, et al. The Pittsburgh Lung Screening Study (PLuSS): outcomes within 3 years of a first computed tomography scan. Am J Respir Crit Care Med. 2008;178(9):956-961. 14. Wilson DO, Ryan A, Fuhrman C, Schuchert M, Shapiro S, Siegfried JM, Weissfeld J. Doubling times and CT screen detected lung cancers in Pittsburgh Lung Screening Study. Am J Respir Crit Care Med. 2012; 185(1):85–89. 15. Pedersen JH, Ashraf H, Dirksen A, et al. The Danish randomized lung cancer CT screening trial: overall design and results of the prevalence round. J Thorac Oncol. 2009;4(5):608-614. 16. Saghir Z, Dirksen A, Ashraf H, Bach KS, Brodersen J, Clementsen PF, D&oslash ssing M, Hansen H, Kofoed KF, Larsen KR, Mortensen J, Rasmussen JF, Seersholm N, Skov BG, Thorsen H, T&oslash;nnesen P, Pedersen JH. CT screening for lung cancer brings forward early disease. The randomised Danish Lung Cancer Screening Trial: status after five annual screening rounds with low-dose CT. Thorax.2012: 67; 296-301. 17. Infante M, Cavuto S, Lutman FR, et al; DANTE Study Group. A randomized study of lung cancer screening with spiral computed tomography: three-year results from the DANTE trial. Am J Respir Crit Care Med. 2009; 180(5):445-453. 18. Lopes-Pegna A, Picozzi G, Mascalchi M, et al; ITALUNG Study Research Group. Design, recruitment and baseline results of the ITALUNG trial for lung cancer screening with low-dose CT. Lung Cancer. 2009; 64(1):34-40. 19. Gutierrez A, suh R, Abtin F, Genshaft S, Brown K. Lung Cancer Screening. Semin Intervent Radiol (2012);30:114-120. 20. Detterbeck FC, Mazzone PJ, Naidich DP, Bach PB. Screening for lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidencebased clinical practice guidelines. Chest. 2013; 143(5):e78S-e92S. 21. Tammemagi MC, Kartki HA, Hocking WG, et al. Selection criteria for lung cancer screening. N Engl J Med. 2013; 368: 728-36. 19 22. Field JK, Oudkerk M, Pederson JH, Duffy SW. Prospects for population screening and diagnosis of lung cancer. Lancet .2013; 382: 732-41. 23. Field JK, Smith RA, Aberle DR, Oudkerk M, Baldwin DR, Yankelevitz D, Pedersen JH, Swanson SJ, Travis WD, Wisbuba II, Noguchi M, Mulshine JL. International Association for the Study of Lung Cancer Computed Tomography Screening Workshop 2011 report. J Thorac Oncol. 2012;7(1):10-9. 24. Xu D, van Klaveren RJ, De Bock GH, Leusveld A, Zhao Y, Wang Y, Vliegenthart R, De Koning HJ, Scholten ET, Verschakelen J, Prokop M ,M Oudkerk. Limited value of shape, margin and CT density in the discrimination between benign and malignant screen detected solid pulmonary nodules of the NELSON trial. Eur Radiol. 2007; 68(2):347-52. 25. Heuvelmans MA, Oudkerk M, De Bock GH, De Koning HJ, Xie X, Van Ooijen P, Greuter M, De Jong PA, Groen H, Vliegenthart R. Optimisation of volume-doubling time cut-off for fast-growing lung nodules in CT lung cancer screening reduces false-positive referrals. Eur Radiol: 2013; 23: 1836-45. 26. Gierada DS, Garg K, Nath H, Fagerstorm RM, Ford MB. CT quality assurance in the lung screening study component of the National Lung Screening Trial: implications for multicenter imaging trials. AJR Am J Roentgenol. 2009; 193(2):419-24. 27. Petrou M, Quint LE, Nan B, Baker LH. Pulmonary nodule volumetric measurement variability as a function of CT slice thickness and nodule morphology. Am J Roentgenol. 2007;188(2):306-12. 28. Wang Y, de Bock GH, van Klaveren RJ, van Ooyen P, Tukker W, Zhao Y, Dorrius MD, Proença RV, Post WJ, Oudkerk M. Volumetric measurement of pulmonary nodules at low-dose chest CT: effect of reconstruction setting on measurement variability. Eur Radiol. 2010; 20(5):1180-7. 29. Revel MP, Merlin A, Peyrard S et al. Software volumetric evaluation of doubling times for differentiating benign versus malignant pulmonary nodules. Am J Roentgenol. 2006; 187:135–142. 30. Gietema HA, Wang Y, Xu D et al. Pulmonary nodules detected at lung cancer screening: interobserver variability of semiautomated volume measurements. Radiology. 2006; 241:251–257. 31. Bach PB, Mirkin JN, Oliver TK, et al. Benefits and harms of CT screening for lung cancer: a systematic review. JAMA. 2012; 307:2418-2429. 32. Midthun DE, Jett JR. Screening for Lung cancer: The US Studies. J Surg Oncol. 2013; 108:275-279. 20 33. Wender R, Fontham ET, Barrera E, Colditz GA, Church TR, Ettinger DS, Etzioni R, Flowers CR, Scott Gazelle G, Kelsey DK, LaMonte SJ, Michaelson JS, Oeffinger KC, Shih Y-CT, Sullivan DC, Travis W, Walter L, Wolf AMD, Brawley OW & Smith RA. American Cancer Society lung cancer screening guidelines. CA Cancer J Clin.2013; 63: 106–117. 34. Jaklitsch MT, Jacobson FL, Austin JH, Field JK, Jett JR, Keshavjee S, et al. The American Association for Thoracic Surgery guidelines for lung cancer screening using low-dose computed tomography scans for lung cancer survivors and other high-risk groups. J Thor Cardiovas Surg. 2012;144(1):33-8. 35. U.S Preventive Services Task Force. Lung Cancer Screening. Recommendation Statement. May/2004. Retrieved from: http://www.uspreventiveservicestaskforce.org/3rduspstf/lungcancer/lungcanrs.htm 36. U.S Preventive Services Task Force. Lung Cancer Screening. Draft Recommendation Statement. Aug/2013. Retrieved from: http://www.uspreventiveservicestaskforce.org/uspstf13/lungcan/lungcandraftrec.htm 37. Taplin SH, Ichikawa L, Yood MU, et al. Reason for late-stage breast cancer: absence of screening or detection, or breakdown in follow-up? J Natl Cancer Inst. 2004;96(20):1518–1527. 38. Coughlin SS, Richardson LC, Orelien J, et al. Contextual analysis of breast cancer stage at diagnosis among women in the United States, 2004. Open Health Serv Policy J. 2009;2:45–46. 39. Mock J, McGhee SJ, Nguyen T, et al. Effective lay health worker outreach and mediabased education for promoting cervical cancer screening among Vietnamese American women. Am J Public Health. 2007;97(9):1693–1700. 40. Meissner HI, Klabunde CN, Han P, Benard V, Breen N. Breast cancer screening beliefs, recommendations and practices: primary care physicians in the United States. Cancer. 2011;117(14):3101–3111. 41. Nadel M, White M. Cancer screening practices frequently deviate from clinical practice guidelines. Ann Fam Med. 2012;10(2):102–110. 42. Nadel MR, Berkowitz Z, Klabunde CN, Smith RA, Coughlin SS, White MC. Fecal occult blood testing beliefs and practices of US primary care physicians: serious deviations from evidence-based recommendations. J Gen Intern Med. 2010;25(8):833–839. 43. Plescia M, White MC. The National Prevention Strategy and breast cancer screening: scientific evidence for public health action. Am J Public Health. 2013;103(9):1545-8. 21 44. National Prevention Council, National Prevention Strategy, Washington, DC: U.S. Department of Health and Human Services, Office of the Surgeon General, 2011. Retrieved from: http://www.surgeongeneral.gov/initiatives/prevention/strategy/introduction.pdf 22