Word - TexasFamiliCare
advertisement

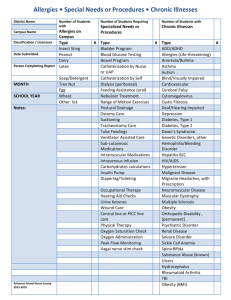
Texas Familicare Medical Group 1725 Chadwick Court, Suite 100 Hurst, Texas 76054 Patients Name:_______________________________________________ Date of Birth:_________________________________________________ Today’s Date:_________________________________________________ FAMILY HISTORY IF ANY BLOOD RELATIVE HAS SUFFERED ANY OF THE FOLLOWING PLEASE CIRCLE AND INDICATE WHICH RELATIVE: M, F, B, S, GM, GF 1) 2) 3) 4) 5) EPILEPSY MIGRAINES MENTAL ILLNESS GLAUCOMA DIABETES 6) THYROID DISEASE 7) HAYFEVER 8) ASTHMA 9) ANEMIA 10) BLEEDS EASILY 11) OSTEOPOROSIS 12) ARTHRITIS 13) HEART DISEASE 14) STROKE 15) HYPERTENSION 16) LIPID DISORDER 17) ALCOHOLISM 18) HEPATITIS 19) CANCER 20) OTHER____________ PATIENT’S MEDICAL HISTORY HOSPITAL ADMISSIONS (NOT INCLUDING PREGNANCIES) YEAR ILLNESS OR OPERATIONS TEST / EXAM LIST ALL MEDICATIONS YOU ARE TAKING INCLUDING: NAME, DOSAGE AND FREQUENCY 1) __________________________________________ 2) __________________________________________ 3) __________________________________________ 4) __________________________________________ 5) __________________________________________ COLONOSCOPY YEAR RECTAL / STOOL CHOLESTEROL EYE EXAM PSA / MALE EXAM VACCINES YEAR TETANUS / TD INFLUENZA (FLU) PNEUMONIA HEPATITIS DO YOU HAVE OR EVER HAD ANY OF THE FOLLOWING: CIRCLE EAR INFECTION-FREQUENT EYE PAIN FAILING VISION DOUBLE OR BLURRED VISION DECREASED HEARING FRACTURE OR DISLOCATION HEAD INJURY NECK INJURY ARM INJURY HAND OR WRIST INJURY SHOULDER INJURY ELBOW INJURY RIB INJURY BACK INJURY LEG INJURY FOOT OR ANKLE INJURY MUSCLE DISORDER AIDS/HIV POSITIVE ALCOHOLISM DRUG ADDICTION VENEREAL DISEASE EPILEPSY CONVULSIONS SKIN DISORDER NOSE BLEEDS-RECURRENT MRSA ABDOMINAL PAIN TUBERCULOSIS APPENDICITIS ANOREXIA DIVERTICULOSIS/CROHN’S/COLITIS ANEMIA BLOOD IN URINE BLOOD DISORDER SUGAR IN URINE ASTHMA/WHEEZING DIABETES BRONCHITIS BLOODY OR TARRY STOOL CHRONIC COUGH DIARRHEA/CONSTIPATION ALLERGIES/HAY FEVER KIDNEY PROBLEM SINUS TROUBLE HERNIA SORE THROAT-FREQUENT STOMACH ULCER RHEUMATIC FEVER CANCER HEART TROUBLE TUMOR / CYST CHEST PAIN ARTHRITIS HIGH BLOOD PRESSURE OSTEOMYELLITIS HEADACHES MYALGIA DIZZY SPELLS NEURITIS FAINTING SPELLS VERICOSE VEINS DIFFICULTY SWALLOWING HARDENING OF ARTERIES NERVOUS DISORDER TUBERCULOSIS FEMALE YEAR WELL WOMENS EXAM MAMMOGRAM PREGNANCIES CHILDREN FOOD OR DRUG ALLERGIES SMOKE START DRINK ALCOHOL START Y/N STOPPED Y/N STOPPED