Appendix 2: Competencies
advertisement

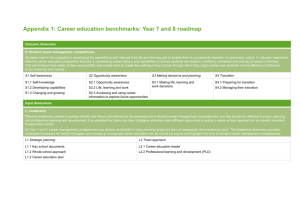
Appendix 2: Competencies Domains of knowledge (Batalden, Berwick et al. 1998) Domain Knowledge 1 Customer/Beneficiary knowledge Identifying customers internal and external to the organisation, describing methods to identify customer needs 2 Health care as a process/system Understanding work as a process and analysing data as a process of work 3 Variation and measurement Collect and analyse data on outcomes of care, interpret qualitative and quantitative data and differentiate common and special cause variation; use data to make changes that decrease unwanted variation 4 Leading, following, making changes Displays skill in active listening, gives and receives constructive feedback 5 Collaboration Work collaboratively with health professionals from other disciplines, work effectively in multi-disciplinary teams, appreciate the importance of multi-disciplinary establishment of organisation-wide quality goals, and know why an interdisciplinary approach is necessary for quality improvement and safety in health care 6 Developing new locally useful knowledge Conduct serial experiments of improvement, ie, PDSA and apply continuous improvement to personal learning and change 7 Social context and accountability Understand the linkage of quality and cost in health care and apply continuous improvement 8 Professional subject matter Gain all the specialist knowledge and skills that equips for competency in quality improvement Quality improvement domains Adapted by the Health Foundation from Batalden & Davidoff 2007 JAMA, cited in Quality Improvement training for health care professionals (The Health Foundation 2012 ). 1 2 3 4 5 Components Examples of topic areas The wider context How the health system is structured and how it works Historical, social and political context within which health systems develop and operate Health policy Accountability Professionalism Psychology of change Learning styles Leadership Teamwork and collaboration Management Multidisciplinary working Reflection and learning from mistakes Seeing health care from then user’s perspective Identifying and targeting the needs and preferences of different subgroups of users Acquiring tools to asses and respond to users Systems thinking Complexity theory and interdependencies Spread Sustainability Planning and predicting Understanding risk and risk management Different forms of evidence The philosophy of science Variation Measurement Local versus generalisable knowledge Small versus large scale change Collecting, analysing and interpreting data Human behaviour Needs and preferences of people who use health services Health care as a process The nature of knowledge Reporting and displaying information Process mapping Leadership for quality (Garman 2011) 1 2 3 4 5 6 Domain Competencies Fosters positive change Advocates and adapts to change ‘Partners’ for change Cultivated a quality-supportive climate Drives for results Verbal communication skills Written communication skills Listening and receiving feedback Educating Strategic planning Strategic thinking and alignment Financial acumen Systems thinking Professional ethics Manages personal limits Resilience and self-restraint Consumer advocacy Future focus Lifelong learning Managing data Analyst thinking/knowledge-based decision-making Develops a knowledge-rich environment Communicating Organisational awareness Self-management Professionalism and professional values Performance improvement Team competencies (Baker, Day et al. 2006) 1 2 3 Teamwork Definition Behavioural examples Team leadership Ability to direct and coordinate the activities of other team member , assess team performance, assign tasks, develop team KSAs, motivate team member, plan and organise and establish a positive atmosphere. Facilitate team problemsolving Provide performance expectations and acceptable interaction patterns Synchronise and combine individual team member contributions Seek and evaluate information that impacts team functioning Engage in preparatory meeting and feedback session with the team Identifying mistakes and lapses in other team members actions Providing feedback regarding team actions in order to facilitate self-correction Recognition by potential backup providers that there is a workload distribution problem in their team Shifting of work responsibilities to underutilised team members Completion of the whole task or parts of tasks by other team members Identify cues that a change has occurred, assign meaning to the change and develop a new plan to deal with changes Identify opportunities for improvement and innovation for habitual or routine practices Mutual performance monitoring (situation monitoring) Backup behaviour The ability to develop common understanding of the team environment and apply appropriate task strategies tin order to accurately monitor teammate performance Ability to anticipant other team member’s needs through accurate knowledge about their responsibilities The ability to shift workload among members to achieve balance during high periods of workload pressure 4 Adaptability Ability to adjust strategies based on information gathered from the environment through the use of compensatory behaviour and reallocation of intra-team resources. Altering a course of action or team repertoire in response to changing conditions 5 6 7 8 Shared mental models Communication (Internal or external Remain vigilance to changes in the internal and external environment of the team. An organising knowledge structure of the relationships between the task the team is engaged in and how the team members will interact Anticipating and predicting each other’s needs Identify changes in the team, task or teammates and implicitly adjust strategies as needed Exchange of information between a sender and a receiver irrespective of the medium Following up with team members to ensure message was received Acknowledging a message as received Clarifying with the sender that the message received is the same as the intended message sent. Taking into account alternative solutions provided by teammates and appraising that input to determine what is most correct Increase task involvement, information sharing, strategizing and participatory goal setting Information sharing Willingness to admit mistakes and accept feedback Team/Collective Propensity to take others’ orientation behaviour into account during the group interactions and the belief in the importance of team goals over individual members’ goals Mutual trust The shared belief that team members will perform their roles and protect the interests of their teammates. Capabilities for individuals (National Advisory Group on the Safety of Patients in England 2013) Berwick’s recommendations for improvement in the NHS link knowledge and skills to specific organisational roles. 1 2 3 4 Domain Competencies Front line staff Setting goals and measures Identifying problems Mapping processes Testing changes Simple waste reduction Simple standardisation Team behaviours Setting goals and measures Identifying problems Mapping processes Sequencing tests of change Simple understanding variation Implementation and spread Simple waste reduction and standardisation Understands systems thinking Leads microsystem Setting goals and measures Identifying problems Implementation of portfolio and management Simple understanding variation Managing spread Simple waste reduction and standardisation Understands microsystems Systems thinking Setting directions and big goals Execution leadership Portfolio selection and management Oversight of improvement Clinical leaders Operational leaders Executives 5 Experts Being a champion and sponsor Understanding variation to lead Analysis, prioritisation of portfolios Deep statistical process control Deep Improvement methods Leadership team advisory re portfolio selection Effective plans to implementation and spread Quality improvement and patient safety skills (The Health Foundation 2014) The most extensive list of knowledge and skills was published in the Building Capability document, Health Foundation. It was gathered from scans of existing quality improvement/safety curricula and programmes. Asterisks (*) indicate safety specific skills. Domains 1 2 Technical safety improvement skills Cause and effect diagrams Process mapping/analysis Identifying where and why improvement is needed; analysing safety risk and measuring/evaluating data, change and outcomes Driver diagrams Swim lane mapping Understanding clinical variation Understanding clinical risk* Proactive risk analysis tools (eg, failure mode and effects analysis)* Model for improvement Identifying error and harm* High reliability systems* Human factors* Root cause analysis Safety-critical work (eg, invasive procedures, infection control, medicines safety, emergencies)* Plan-Do-Study-Act (PDSA) rapid improvement cycles Value stream mapping Spaghetti diagrams Fishbone analysis Five whys Recognising, reporting and managing adverse events and near misses* Patient stories Measurement skills Measurement for improvement Designing measures and evaluating data, change and outcomes Setting baselines Excel, Pareto, Run, SPC, Win Charts Balanced scorecards Quality measurement Collecting data/audit 3 4 Data sampling Analysing data Safety culture measures (eg, safety culture interaction)* Measurement of reliability Mortality measures* Harm measures* Patient experience measures Evaluating improvement Engagement and implementation skills Leading change/improvement Understanding others’ perspectives Influencing and engaging colleagues in patient safety work; involving staff, patients and partners; motivating those involved to change/enhance practice and sustain change over time Creativity and innovation Sustainability Organising for quality Staff engagement Group facilitation skills Creating a culture for improvement/safety* Working in partnership Patient and carer engagement Coaching principles and practice OD cycle and skills (contracting, data collection, data feedback, implementation) Effective teams Team diagnostic tools (e.g. Aston organisation development) Motivation theory Communicating about risk, safety and errors* Learning and changing practice from errors* Manchester Patient Safety Framework (MPSF)* S-BAR handover tool Handling conflict effectively Respectful and non-respectful behaviours Research and learning skills Qualitative research methods Quantitative research methods Extending and deepening knowledge and understanding about safety improvement; sharing learning; Research findings into practice Peer reviewed publishing 5 applying and transferring research into practice across wider contexts Conducting patient safety research* Action research Systems leadership skills Whole systems theory Social movement theory Creating a culture of values and behaviours which nurture and promote safety improvement across a meso- or macro-system Understanding complex systems Leading change across organisational boundaries Developing shared purpose and values Latent conditions for safety Peer leadership across systems Patient safety competencies (The Safety Competencies Steering Committee 2008) Canadian patient Safety Institute (The Safety Competencies Steering Committee 2008) identified six competencies required for ensuring patient safety: Each Domain is further specified by key competencies and enabling competencies. This table will include only the key competencies for each domain. 1 2 3 4 5 Domain Description Contribute to a culture of patient safety Commit to patient and provide safety through safe, competent high quality daily practice Describe the fundamental elements of patient safety Maintain and enhance patient safety practice through ongoing learning Demonstrate a questioning attitude as a fundamental aspect of professional practice and patient care Participate effectively and appropriately in an interprofessional health care team to optimise patient safety Meaningfully engage patients as the central participants in their health care teams Appropriately share authority, leadership and decisionmaking Work effectively with other health care professionals to manage inter-professional conflict Demonstrate effective verbal and non-verbal communication abilities to prevent adverse events Communicate effectively in special high risk situations to ensure the safety of patients Use effective written communications for patient safety Apply communication technologies appropriately and effectively to provide safe patient care Recognise routine situations and settings in which safety problems may arise Systematically identify, implement and evaluate context-specific safety solutions Anticipate, identify and manage high risk situations Describe the individual and environmental factors that can affect human performance Apply techniques in critical thinking to make decisions safely Appreciate the impact of human/technology interface in Working in teams for patient safety Communicating effectively for patient safety Managing safety risks Optimising human and environmental factors safer care 6 Recognise, respond to and disclose adverse events Recognise the occurrence of and adverse event or close call Mitigate harm and address immediate risks for patients and others affected by adverse events and close calls. Disclose the occurrence of an adverse event to the patient and/or their whānau/family as appropriate and in keeping with relevant legislation Report the occurrence of an adverse event or close call Participate in timely event analysis, reflective practice and planning for the prevention of recurrence