P. Indira 1 , S. Jyotsna 2 - journal of evidence based medicine and
advertisement

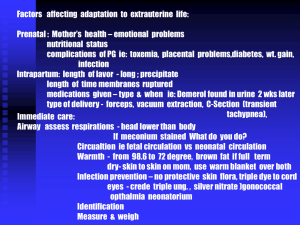
DOI: 10.18410/jebmh/2015/759 ORIGINAL ARTICLE HYPOGLYCEMIA AMONGST NEONATES ADMITTED IN NICU IN A TERTIARY CARE CENTRE KGH P. Indira1, S. Jyotsna2 HOW TO CITE THIS ARTICLE: P. Indira, S. Jyotsna. “Hypoglycemia Amongst Neonates Admitted in NICU in A Tertiary Care Centre KGH”. Journal of Evidence based Medicine and Healthcare; Volume 2, Issue 35, August 31, 2015; Page: 5465-5471, DOI: 10.18410/jebmh/2015/759 ABSTRACT: Hypoglycemia is a historically one of the most common metabolic problem seen in both the newborn nursery and NICU but confirming a diagnosis of clinically significant hypoglycemia requires to be investigated. OBJECTIVES: to study incidence of hypoglycemia in NICU, various factors associated with hypoglycemia, clinical features of hypoglycemia. MATERIALS AND METHODS: Study Design: A hospital based prospective study conducted Neonatal Intensive Care Unit, Department of pediatrics, King George Hospital. For a period of 4 months (Jan 2015-April 2015) were 300 new born babies were included. RESULTS: 1) Distribution of hypoglycemia in study group are 95% normoglycemic; 5% hypoglycemic. 2) Among the total babies enrolled % of hypoglycemia in male babies 3% and female babies 2%. 3) Percentage of hypoglycemia among the birth weight <2500gm is 9.1% when compared to >2500gms which is 2.2%. CONCLUSIONS: There is statistical significant association between hypoglycemia and gender i,e p=.04. There is statistically significant association between hypoglycemia and birth weight of the baby i, e p=.01. Further study recommended as our study duration was short and number of babies enrolled are also less. KEYWORDS: Hypoglycemia, Birth weight, Newborn. INTRODUCTION: Hypoglycemia in a neonate has been defined as blood sugar value < 40mg/dl. Hypoglycemia is encountered in a variety of neonatal conditions including prematurity, growth retardation and maternal diabetes. Screening for hypoglycemia in certain high-risk situations is recommended. Supervised breast-feeding may be an initial treatment option in asymptomatic hypoglycemia. However, symptomatic hypoglycemia should always be treated with a continuous infusion of parenteral dextrose. Neonates needing dextrose infusion rates above 12 mg/kg/min should be investigated for the cause of hypoglycemia. Hypoglycemia has been linked to poor neuro-developmental outcome, and hence aggressive screening and treatment is recommended.1,2 Further descriptions of the neurological sequelae associated with symptomatic hypoglycemia in the newborn period followed. Concern arouse that hypoglycemia without clinical signs might also lead to neurodevelopmental sequelae.3,4 In Tanzer F et al study ( in full term neonates) , lowest blood glucose level was seen in the first 3 hours of life5. METHODS: Design and Setting: This prospective study has been carried out in Neonatal Intensive Care Unit, Department of Pediatrics King George Hospital, Vishakhapatnam over a period of 4 months from January 2015 to April 2015. Study Population: Total number of babies enrolled were 300. J of Evidence Based Med & Hlthcare, pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 2/Issue 35/Aug. 31, 2015 Page 5465 DOI: 10.18410/jebmh/2015/759 ORIGINAL ARTICLE Inclusion Criteria: Inborn babies in King George hospital brought to our NICU. Exclusion Criteria: All out borns. Data Collection: Blood glucose estimated by one touch basic glucometer. Immediately within an hour after birth-repeat after two and four hours of admission. In high risk neonates blood glucose 4-6 hourly for next 48 hours. Blood glucose levels of less than 40mg/dl considered as hypoglycemia irrespective of gestational age and birth weight.6 Enteral feeding within half an hour of birth was started (Intravenous glucose only when weight of babies was <1500gms or in sick neonates). OBSERVATIONS: Total 300 babies were enrolled in the study, the following observations were grouped into Group A and B as hypoglycemic (15) and normoglycemics;285 respectively Group A: Hypoglycemia (< 40 mg/dl) N=15. Group B: Normoglycemia (> 40mg/dl) N=285. Following observations are reported in our study. Figure 1: Total babies enrolled were 300 5% of babies are hypoglycemic and 95% of babies are normoglycemic. J of Evidence Based Med & Hlthcare, pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 2/Issue 35/Aug. 31, 2015 Page 5466 DOI: 10.18410/jebmh/2015/759 ORIGINAL ARTICLE Figure 2 p=0.04, there is statistical significant association between hypoglycemia and gender. Figure 3 p =0.01 there is statistically significant association between hypoglycemia and birth weight of the baby.7 J of Evidence Based Med & Hlthcare, pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 2/Issue 35/Aug. 31, 2015 Page 5467 DOI: 10.18410/jebmh/2015/759 ORIGINAL ARTICLE Figure 4 Among the hypoglycemic 73% of the babies shown symptoms of hypoglycemia. Risk factor Total babies No. of babies showing Septicemia 50 4(8%) Normal babies(hypothermic) 65 2(3%) Respiratory distress 40 1(2.5%) Birth asphyxia 35 2(5.7%) Tabular form showing the risk factors in hypoglycemic infants: term babies: Total 205 babies preterm babies Total 95 babies Small for gestation 55 1(1.8%) Respiratory distress 40 0% Tabular form showing the risk factors in hypoglycemics infants J of Evidence Based Med & Hlthcare, pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 2/Issue 35/Aug. 31, 2015 Page 5468 DOI: 10.18410/jebmh/2015/759 ORIGINAL ARTICLE Figure 5 Refusal of feeds was the most common sign among the hypogylcemics. hypoglycemics normoglycemics Preterm 6 89 Term 9 196 Total 15 285 Total 95 205 300 Table 1: Showing the percentage of pre-terms and term babies with hypoglycemia hypoglycemia within 24hrs 10 babies 3.33% hypoglycemia >24hrs 5 babies 1.66% Tabular showing hypoglycemia onset timing DISCUSSION: Neonatal hypoglycemia is one of the most common problems seen in neonatal intensive care units. It is accepted that the persistent early and prolonged hypoglycemia results in brain damage and mental retardation.8 Thus, neonatal intensive care therapy units must identify all neonates with risk of neonatal hypoglycemia, and to early initiate the treatment, because early recognition offers the best outcomes. In the present the accepted definition of hypoglycemia is whole-blood glucose level<40mg/dl, both in the term neonates and in the premature infants. J of Evidence Based Med & Hlthcare, pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 2/Issue 35/Aug. 31, 2015 Page 5469 DOI: 10.18410/jebmh/2015/759 ORIGINAL ARTICLE The risk category of newborns with neonatal hypoglycemia: Premature infants. Small for gestational age infants. Large for gestation age infants. Post maturity. Twins. Infant of diabetic mother. Infants born from mothers who receive high glucose infusion before delivery. Newborn with neonatal pathology. OTHERS: Beck with weidemann syndrome, erythro-blastosis, wrong-positioned umbilical artery catheter. The results of our study suggest that newborns with low body weight are at greater risk for hypoglycemia. The small for gestation age preterm neonates are at greater risk of neonatal hypoglycemia, because the fuels are directed towards growth, as opposed to glycogen deposits.9 P. K Singhal et.al9 study showed 71.5% case were term birth asphyxia with hypoglycemia and study showed 11.6% septicemia cases developed hypoglycemia comparison to our study showed 5.7% and 8% respectively. Our study is comparable to study done by M.A.Bhat et al10 in SGA babies, 98% of the episodes of hypoglycemia occurred within 24hrs. Acc to Hawdon et al11 study on preterm infants the mean blood glucose concentration was significantly lower on the 1st day than on the subsequent days. CONCLUSION: Hypoglycemia is a common preventable and neglected problem in developing countries. Our study showed that preterm, LGA’s, SGA’s term, birth asphyxia, IGDM/IDM’s septicemia, hypothermia are at an increased risk of developing hypoglycemia. More than half of the cases were asymptomatic even though the blood glucose levels showed hypoglycemia. Hence these categories of neonates deserve an aggressive blood sugar monitoring and management in order to reduce the early infant mortality and neuro development sequelae in later lofe. Irrespective of the symptomatic and asymptomatic newborns has to be screened for blood glucose level within 72 hours which can prevent hypoglycemia in turn can prevent tissue damage. REFERENCES: 1. Ashish jain, Rajiv Aggarwal M, Jeeva sankar, vinod k paul AIIMS protocols neonatology, New Delhi page no: 221. 2. Williams AF. Hypoglycemia in newborns: a review. Bull. World Health Organ. 1997; 75: 261290. 3. Meherban Singh Care of the new born, 8th edition pg no 466 4. Christine A gleason, sherin u devaskar Averys diseases of the newborn 9th edition pg no 1322. 5. Kalhan S, Peter-Wohl S. hypoglycemia: what is it for the neonate? Am J Prenatal 2000; 17: 11-4. J of Evidence Based Med & Hlthcare, pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 2/Issue 35/Aug. 31, 2015 Page 5470 DOI: 10.18410/jebmh/2015/759 ORIGINAL ARTICLE 6. Duvanel CB, et al. long term effects of neonatal hypoglycemia on brain growth and physchomotor development in small for gestational age preterm infants. J Pediatrics 1990; 134: 492-8] 7. Tanzer F, Yanzar N, Yazar H, et al: Blood glucose levels and hypoglycemia in full term neonates during the first 48hours of life. J. Trop Pediatr. 1997; Feb; 43(1): 58-60. 8. Leeuw RD, de Vries IJ. Hypoglycemia in small–for-dates new born infants, Pediatrics 1976, 58: 18-22. 9. Singhal P.K,.Singh M, Paul V.K, Deodari A.K, Ghorpade M.G, Malhotra A. Neonatal Hypoglycemia-Clinical profile and glucose requirements. Indian. Pediatrics 1992; 29: 167-71 10. Bhat MA. Hypoglycemia in small for gestational age babies. Ind. J. Pediatrics. 2000; 67(6):423-427. 11. Hawdon JM. Patterns of metabolic adaption for pre-term infants in the first neonatal week. Arch. Dis. Chil. 1994; 70: F60-F65. AUTHORS: 1. P. Indira 2. S. Jyotsna PARTICULARS OF CONTRIBUTORS: 1. Assistant Professor, Department of Pediatrics, Andhra Medical College, Vizag, Andhra Pradesh. 2. Post Graduate, Department of Pediatrics, Andhra Medical College, Vizag, Andhra Pradesh. NAME ADDRESS EMAIL ID OF THE CORRESPONDING AUTHOR: Dr. P. Indira, Plot No. 26, Palace Compound, Pedha Waltair, Visakhapatnam-17. E-mail: indiraguda07@gmail.com Date Date Date Date of of of of Submission: 21/08/2015. Peer Review: 22/08/2015. Acceptance: 24/08/2015. Publishing: 31/08/2015. J of Evidence Based Med & Hlthcare, pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 2/Issue 35/Aug. 31, 2015 Page 5471