Patient Registration and Medical History Form
advertisement

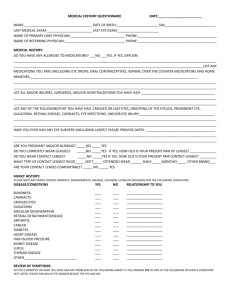
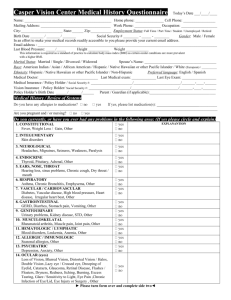
Patient Registration & Medical History Form (Please be sure to bring your Medical Insurance Card, any Eyewear, Contact Lenses, and Contact Solution) First Name: __________________Last Name: ____________________ Middle Initial: ___ Preferred Name: _____________ Birth Date: ______________ Social Security Number: ________________ Sex: M / F Marital status: Single Married Other Address: ____________________________________________ City:______________________ State: _______ Zip:____________ Which phone number do you prefer? Home Work Cell Home #____________ Work #____________Cell #______________ Email address: _____________________________________Occupation: How did you hear about us? ______________________________ _Referred by: ________________________ ____ Family Members: __________________________________________ Are they patients at this office? _______________________ Hobbies: _____________________________________________________________________________ ________ Insurance Information Primary Medical Insurance: Vision Insurance:_______________________________________ Policy Holder’s Name: Policy Holder’s Social Security Number: ____________________ Policy Holder’s Birth Date: Policy Holders Employer: ___________________ __________ Reason For Visit How can we help you today? In this space please check/explain any signs and/or symptoms you are experiencing. Loss of vision Dry eyes Light sensitivity Sandy/gritty feeling Floaters Blurred vision Red eyes Tired eyes Eye pain/soreness Crossed eyes Double vision Burning/itching Glare Watery eyes Flashes of light Other:_____________ Patient History Last Medical Exam:_______________________________Physician/Clinic:__________________________________________ Have you had any surgeries, major injuries, or hospitalizations? Y / N____________________________ Do you smoke? Y N How much per month? _________Do you consume alcohol? Are you interested in LASIK surgery? Y __ Y N If yes, how much? __ _ _ N Last Eye Exam (estimate):___________________________ _ Where:___ _________________________ Glasses: Do you currently wear glasses? Y N Contact Lenses: Do you wear contact lenses? Y N What type of contact lenses do you wear? What is the brand? _______________What are the powers of your contact lenses? Soft Rigid Right:_________ Left:_________ How old is your current pair of contact lenses? ______ Weeks/ Months / Years Do you sleep in your contact lenses? Y How often do you replace your contact lenses? Daily What solutions do you use with your contact lenses? 2 weeks Renu Optifree Monthly N Other:______________ Revitalens Biotrue Clear Care Other Are you taking any medications: Y / N Please List: ____________________________________________________________ ________________________________________________________________________________________________________ Do you have any allergies to medications: Y / N List: ___________________________________________________________ List any other allergies: ___________________________________________________________________________________ Family History Has anyone in your family been diagnosed with any of the following (check all that apply): No problems Diabetes High blood pressure Heart Disease Cancer Thyroid Issues Has anyone in your family been diagnosed with any of the following eye problems (check all that apply): No problems Glaucoma Amblyopia (lazy eye) Strabismus (eye turn) Cataracts Retinal Detachment Macular degeneration Review of Systems Please circle the condition(s) that you have. All of these may affect the health of your eyes. Ocular (Eye) Constitutional Ear/Nose/Mouth/Throat Glaucoma Amblyopia (Lazy Eye) Cataract Inflammatory Disorder Dry Eye Retinal problems Macular Degeneration Strabismus (Eye Turn) Fever Weight Loss/Gain Cancer Fatigue Syndrome Developmental Disability Sinus Congestion Laryngitis Dry Mouth Hearing Loss Sinusitis Neurological Psychiatric Cardiovascular Migraines Cerebral Palsy Multiple Sclerosis Tumor Epilepsy Stroke/CVA Depression Anxiety Attention Deficit Disorder Bipolar Disorder Vascular Disease Stroke Congestive Heart Failure Heart Disease High Blood Pressure Respiratory Gastrointestinal Genitourinary Emphysema Bronchitis COPD Asthma Sleep Apnea Colitis Crohn’s disease Ulcer Irritable Bowel Syndrome Acid Reflux Celiac Disease Prostate Disease/Cancer STD Kidney Disease Nursing Pregnant Benign Prostate Hypertrophy Musculoskeletal Integumentary (Skin) Endocrine Ankylosing Spondylitis Fibromyalgia Muscular Dystrophy Osteoarthritis Osteoporosis Gout Rosacea Psoriasis Eczema Herpes Simplex/Cold Sores Herpes Zoster/Shingles Insulin Dependent Diabetes (Type I) Non-Insulin Diabetes (Type II) Hormonal Dysfunction Thyroid Dysfunction (Hypo/Hyper) Blood/Lymph Allergy/Immunologic Other: Please list Anemia Large volume blood loss Ulcer High Cholesterol Rheumatoid Arthritis Lupus Allergies: Drug/ Environmental Sjogren’s Syndrome NOTICE OF PRIVACY PRACTICES: I have been shown or offered a copy of Precision Eye Care’s statement on privacy policies that is displayed at our front desk. AUTHORIZATION TO RELEASE INFORMATION: I hereby authorize Precision Eye Care, LLC to release any medical or incidental information that may be necessary for medical benefit in processing applications for financial benefit. This includes, but is not limited to, my insurance company, rehabilitation services, social security administration, and worker’s compensation. CONSENT FOR TREATMENT: I hereby authorize Precision Eye Care, LLC to administer diagnostic and medical procedures as may be necessary for proper health care. OFFICE POLICY ON PAYMENT: I understand that I am responsible for payment of all charges. As a courtesy, my insurance will be billed for me. It is my responsibility to pay any deductible, co-pay or any other balance not paid by my insurance company. I authorize insurance benefits to be paid directly to the provider. I understand that any remaining balance on my account after 30 days will accrue interest at an annual rate of 18% and that I will be responsible for any reasonable costs associated with the collection of past-due balances. VISION PLAN COVERAGE: I understand that only one vision plan may be used for exam/materials per visit, per patient and that the vision plan to be used must be chosen before the exam occurs and cannot change at a later date. ___________________________________________ PRINTED NAME OF PATIENT OR PATIENT REPRESENTATIVE _______________________________________ DATE ______________________________________________________ SIGNATURE ________________________________________ RELATIONSHIP TO PATIENT