Health History Questionaire
advertisement

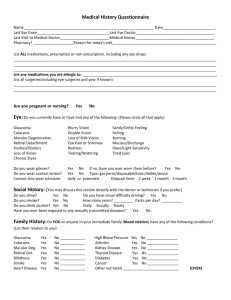
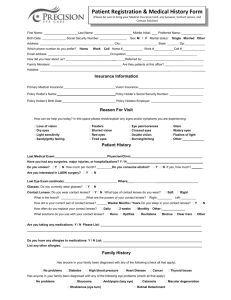
Casper Vision Center Medical History Questionnaire Today’s Date ___/____/____ Name: ______________________________________________ Home phone: _______________ Cell Phone: _________________ Mailing Address: _____________________________________ Work Phone: ______________ Occupation: ___________________ City:______________________ State:______ Zip:___________ Employment Status: Full Time / Part Time / Student / Unemployed / Retired Birth Date _______ / _______ / _______ Social Security # ________ - _____ - ________ Gender: Male / Female In an effort to make your medical records readily accessible to you please provide your current email address. Email address : _______________________________________________________________________________________________ Last Blood Pressure: _____/_____ Height ___________ Weight ____________ This information is required as a standard of practice to calculate body mass index (BMI) as certain ocular conditions are more prevalent with a higher BMI. Marital Status: Married / Single / Divorced / Widowed Spouse’s Name: ______________________________________ Race: American Indian / Asian / African American / Hispanic / Native Hawaiian or other Pacific Islander / White (European) / __________ Ethnicity: Hispanic / Native Hawaiian or other Pacific Islander / Non-Hispanic Preferred language: English / Spanish Medical Doctor: _______________________________ Last Medical exam: _____________ Last Eye Exam: __________________ Medical Insurance / Policy Holder / Social Security #: ______________________/_________________________/_______-____-______ Vision Insurance / Policy Holder/ Social Security #: ______________________/_________________________/_______-____-_______ Policy Holder’s Birth Date ______/_______/______ Parent / Guardian (if applicable):___________________________________ Medical History / Review of Systems __________ ____________________________________________________________________________________________________________ Are you pregnant and / or nursing? Do you currently, or have you ever had any problems in the following area: (If yes please circle and explain) 1. CONSTITUTIONAL Fever, Weight Loss / Gain, Other 2. INTEGUMENTARY Skin disorders 3. NEUROLOGICAL Headaches, Migraines, Seizures, Weakness, Paralysis 4. ENDOCRINE Thyroid, Pituitary, Adrenal, Other 5. EARS, NOSE, THROAT Hearing loss, sinus problems, Chronic cough, Dry throat / mouth 6. RESPIRATORY Asthma, Chronic Bronchitis, Emphysema, Other 7. VASCULAR / CARDIOVASCULAR Diabetes, Vascular disease, High blood pressure, Heart disease, Irregular heart beat, Other 8. GASTROINTESTINAL GERD, Diarrhea, Stomach pain, Vomiting, Other 9. GENITOURINARY Urinary problems, Kidney disease, STD, Other 10. MUSCULOSKELATAL Rheumatoid arthritis, Muscle pain, Joint pain, Other 11. HEMATOLOGIC / LYMPHATIC Blood disorders, Leukemia, Anemia, Other 12. ALLERGIC / IMMUNOLOGIC Seasonal allergies, Other 13. PSYCHIATRIC Depression, Anxiety, Other 14. OCULAR (eyes) Loss of Vision, Blurred Vision, Distorted Vision / Halos, Double Vision ,Lazy eye / Crossed eye, Drooping of Eyelid, Cataracts, Glaucoma, Retinal Disease, Flashes / Floaters, Dryness, Redness, Itching, Burning, Excess Tearing, Glare / Sensitivity to Light, Eye Pain ,Chronic Infection of Eye/Lid, Eye Injury or Surgery , Other ► Please turn form over and complete side two◄ EXPLANANTION List any medications you take (including oral contraceptives, aspirin, over the counter medications and home remedies): ____________________________________________________________________________________________________________ ____________________________________________________________________________________________________________ ____________________________________________________________________________________________________________ ____________________________________________________________________________________________________________ List all major injuries, surgeries and / or hospitalizations you have had: __________________________________________________ ____________________________________________________________________________________________________________ ____________________________________________________________________________________________________________ Do you wear glasses? Do you wear contact lenses? If yes, check type of contact lens Social History Rigid Soft Other What brand of soft contact lenses are you wearing? _______________ This information is kept strictly confidential. However, you may discuss this portion directly with the doctor if you prefer. Yes, I would prefer to discuss my Social History information directly with my doctor. (Check Box) Do you drive? If yes, do you have visual difficulty when driving? If yes, please describe: ____________________________________________________________________________________________________________ Do you use tobacco products? Do you drink alcohol? Do you use illegal drugs? If yes, type / amount / how long: __________________________________________ If yes, type / amount / how long: ________________________________________________ If yes, type / amount / how long: ______________________________________________ Have you ever been exposed to or infected with: Gonorrhea Hepatitis HIV Syphilis Family History Please note any family history (parents, grandparents, siblings, children, living or deceased) for the following conditions: DISEASE / CONDITION NO YES ? RELATIONSHIP TO YOU Blindness Eye turn / Crossed eye Glaucoma Macular degeneration Retinal Detachment / Disease Arthritis Cancer Diabetes Heart Disease High Blood Pressure Kidney Disease Lupus Thyroid Disease Other ____________________ This space is provided for you to list any condition not listed or comments that you think the doctor should be aware of. ____________________________________________________________________________________________________________ ____________________________________________________________________________________________________________ PAYMENT POLICY: The exam fee is to be paid the day of the exam. The balance is due when the glasses or contact lenses are dispensed. Referred By: __________________________________________________________________ **Unless specified to our receptionist, a text message will automatically be sent as a reminder for any future office visits scheduled.** Patient’s / Guardian’s Signature _________________________________________________________ Date _________________ Doctor’s signature ____________________________________________________________________ Date _________________