Contracting models Key benefits Key risks As
advertisement

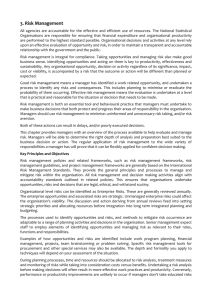
Contracting models Key benefits As-is (Do nothing option) Informal network approach with profit / risk sharing Accountable Care Organisation (ACO) Integrated Care Hubs (Prime Provider model) Key risks • System and relationships already in place • No costs (HR/VAT) associated with implementation • Unable to support transformational change • Inability to move funding around the system • Current system and relationships could be ‘geared up’ to implement this model relatively easily • No costs (HR/VAT) associated with implementation • Ability to share profits may be limited based on need to make savings within QIPP and may encourage adverse competition • Arrangements are non-statutory and potentially unsustainable, e.g. uncertain governance arrangements for dealing with any deficits • Complex contracting processes with multiple organisations • All providers brought together contractually within a single ACO • Goals are focused around the achievement of an agreed set of balanced scorecard objectives • No costs (HR/VAT) associated with implementation • Evidence from the USA suggests model can improve quality of care and lower costs • May be difficult for providers to show evidence of achievement of balanced scorecard objectives • Works best where providers are given a pooled budget for integrated care • Need to move towards payments based on risk/ outcomes rather than fee-for-service (PBR) • A single provider takes all responsibility for providing care within a pathway, therefore contracting is straightforward • No organisational change required, assuming an existing provider becomes the prime provider • Ability to identify/ agree an existing or new local provider who can take on this accountability • Requires true integration across providers, e.g. information sharing and culture change (staff to think of themselves as a unified organisation) • May be costs (HR/VAT) associated with implementation if any staff move across to the prime provider Key benefits Key risks Alliance • Collaborative approach with • Contracts for the formation of the all organisations alliance are usually time-limited, (commissioners and therefore may not be sustainable providers) sharing • No evidence of application in UK contractual responsibility health/ social care context, and may and risk, therefore promotes require changes to the regulatory joint ownership of outcomes environment to implement this model • No organisational change (however has been used in New required, except to put in Zealand and in UK infrastructure place a contract for the projects) alliance and governance arrangements for working together. • Can be implemented quickly, with contracts amended as the project, risks or scope develops • No costs (HR/VAT) associated with implementation Single Integrated Care Organisation • Clear accountability and contracting arrangements. • Sustainable over the longer term • Would promote culture change and information sharing Joint Venture with Joint Management Board of providers • Collaborative approach • Ability of staff in each provider between providers, organisation to work in a truly promoting joint ownership of integrated/ joined-up way outcomes and accountability, and shared risk • More sustainable than an alliance (which tends to be time-bound) • No organisational change required, except to put in place the JMB and contracts with this organisation • No costs (HR/VAT) associated with implementation • Used in other UK health/ social care settings (e.g. Lewisham) • Would require a long period for implementation, supported by consultation and legislation • Costs (HR/VAT) of implementation where staff move across to the new organisation (whether NHS or LA) Key benefits Key risks Principal provider (contractor) and subcontracting model (Prime Vendor or Prime Contractor model) • A single provider takes a responsibility for providing or sub-contracting care within a pathway • No organisational change required, assuming an existing provider becomes the principal provider, and all other existing providers can play a role in care provision • No costs (HR/VAT) associated with implementation • Extensive contracting arrangements required within and between principal and prime contractors • Mixed levels of risk, with principal providers taking on most risk Capitated outcomes based contracts (COBICs) • Incentivises performance by • Performance incentives may linking payment to outcomes encourage adverse competition • Collaborative approach, • Absence of a defined structure brings particularly around risk reliance on good relationships sharing between partners, therefore may not • No organisational change be sustainable required • Difficult contracting arrangements as • Links well with the desire to each entity is responsible for move to a capitation funding delivering its own services but jointly model (see later) accountable for the delivery of outcomes • Requires understanding of total spend in order to calculate capitations Funding models Key benefits Key risks Payment by Results • Encourages organisations with above average costs to lower these towards the average • Helps to promote provider productivity • Some scope for varying national prices to promote innovation and integrated care • Easy to implement as system is already in place • Places greater focus on the use of specialist care, therefore may detract investment from preventative and community based approaches • Based around rewarding activity rather than outcomes • Does not encourage generation of savings across the system, risk sharing or integrated care • Current system works best for most providers, who may be unwilling to move away from this approach Block/ rolling contracts • Promotes stability for commissioners and providers as budget is set at the start of the year • May encourage providers to innovate when working in a fixed budget • Does not incentivise productivity or savings across the system • Value of contract is not usually linked to the level of needs/ risk within the local population Key benefits Key risks Capitation • Assists in avoiding inappropriate use of specialist care by encouraging the system to innovate and share risks • Can be used to specify desired outcomes for a specific disease or pathway group, and expanded if successful • Approach has been tried and tested in Kaiser Permanente • Complex to develop for local population, particularly when a risk profile is used • Implementation of this model requires providers to be integrated or working in an integrated way Cap and collar • Promotes stability for • May require providers to take a commissioners and greater share of the risks providers as budget is set at • Value of contract is not usually linked the start of the year to the level of needs/ risk within the • Could provide an interim local population solution as it is relatively easy to implement, whilst moving to a more sophisticated model based on need • May encourage providers to innovate whilst also incentivising productivity and savings in the system Pooled budgets • Promotes integrated working • Overspend may occur and dealing • Assists with expenditure with this could be difficult if partner control and helps to avoid priorities change ‘cost shunting’ • Value of contract is not usually linked • Relatively straightforward to to the level of needs/ risk within the implement local population Aligned budgets • Flexible approach which can • More bureaucratic than a pooled be used outside of formal budget partnerships and when there • Does not promote more integrated is a possibility of overspend, working cost-shunting or changing • Value of contract is not usually linked priorities to the level of needs/ risk within the • Relatively straightforward to local population implement Reproduced from West Cheshire, Community Budget programme Cited in GM Community Budgets Programme Health and Social Care Theme Narrative Report 2012-11-12 Incentives and Delivery Vehicles A key argument of this report is that new models of integrated care are required, shifting the focus from episodic and reactive to population-based and planned care. Although there will be different approaches to integrated care within GM (reflecting the different local contexts and circumstances), many of the critical success factor and barriers are likely to be similar. The issues of common purpose, culture and leadership are dealt with elsewhere in the report. Given the ambition to substantially reduce unplanned admissions to hospital and care homes, the issue of financial risks and incentives is critical because they are powerful drivers that can align, or generate dysfunctional, organisational behaviour. The NHS tariff is largely designed to reward growth and support the delivery of timely and efficient care. It is not designed to reward providers to manage demand or reduce their activity; NHS providers primarily get paid for treating patients not for preventing hospitalisation. This is not to say that hospitals can’t or haven’t played a role in managing demand however this has tended be a marginal role and often despite (not because of) economic incentives. There is a variety of alternative contracting and payment regimes that could be adopted (see below and Appendix IV) to incentivise this approach, though the complexity of this task should not be underestimated. Particular attention will need to be paid to unintended consequences. For example, crude block contracts (where a provider is paid a fixed fee for a defined range of services), transfer the risk of managing excess demand from commissioner to provider and could lead to inappropriate under-treatment. Many integrated care systems operate with some form of a capitated budget, creating incentives to keep people well. Some of the US accountable care organisations have identified more sophisticated approaches, combining elements of condition-specific or full capitation, along with pay-for-performance. Payment for whole care episodes and ‘year-of-care’ for some long term conditions have also been piloted in mainland Europe and are currently being developed in the UK. There is a spectrum of potential organisational models that could be pursued, from formal merger down to simply sharing of information. Most interest in GM is associated with models of integrated working that stop short of full merger. Indeed, there is no “perfect” organisational model - it is likely that different models or approaches will be required in different circumstances. Risk and benefit sharing is likely to be critical to the success of integration, though its precise form depends crucially on the mechanisms used to deliver integrated care. Most organisations want to be part of the ‘future’ and therefore models of care that result in a wholesale transfer of care from one party to another are likely to result in some resistance (whether active or passive). Often multiple organisations will have responsibility for providing care; hence wherever possible payment systems should support and incentivise shared care and joint outcomes. Arrangements that allow multiple parties to have a ‘stake’ in the solutions that are created are more likely to act as both an incentive for implementing the required changes and ensuring the agreed outcomes are achieved. A related issue is the basis upon which costs are extracted, given the significant fixed costs within acute providers. The simplest approach is to ensure that any reduction of provider income (associated with changes in activity) is determined by a transparent and robust assessment as to the ability to extract costs rather than using tariff. The ability to extract costs will largely be determined by the scale and nature of activity reduction. Most acute costs are associated with inpatient activity where a single ward is effectively the minimum unit of currency. Where there are timing differences between activity (income) and cost reductions, transitional non-recurrent funding could be used in-year. Whilst the approach minimises risks to providers (avoid destabilising the system), the downside is that without sufficiently large scale interventions which enable semi fixed costs to be released, and it will be difficult to deliver substantial cashable savings. Jack Sharp 2012 Taken from GM Community Budgets Programme Health and Social Care Theme Narrative Report 2012-11-12