View - aoahyderabad2015
advertisement

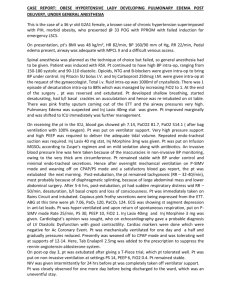
MANAGEMENT OF A CASE OF PERIPARTUM DILATED CARDIOMYOPATHY POST- EMERGENCY LSCS BACKGROUND : Peripartum cardiomyopathy is defined as the onset of acute heart failure without demonstrable cause in the last trimester of pregnancy or within the first 6 months after delivery. We are reporting a case of peripartum cardiomyopathy,after emergency caesarean section developed ventricular arrhythmias and cardiac arrest during surgery. CASE PRESENTATION : A 25-yr old female , primigravida, at 36weeks of gestation, an un-booked case , presented to the labour room with history of seizures and 1 episode of vomiting since 3hrs. On Pre-anesthetic evaluation : Patient was irritable and semi-conscious. pulse:110/minute, blood pressure:190/110 mm of Hg, SPO2 : 57% with 8litres of oxygen, cardiovascular system: s1 ,s2 heard,no murmurs, respiratory system: bilateral crepitations present, per abdomen: term size uterus, ECG showed no significant changes. Patient pre-medicated with Inj.glycopyrolate 0.2mg/iv, Inj.Ondansetron 4mg/iv,Inj.Fentanyl 100mcg/iv, pre-oxygenated with 6ltrs Oxygen.Rapid sequence induction done with Inj.Propofol 100mg/iv. Intubation was facilitated by Inj.SuccinylCholine 100mg intravenously and intubated orally by direct laryngoscopy with 7.5mm size cuffed Endotracheal tube. Soon after intubation Patient developed asystole. Chest compressions started in left lateral position.Inj.Adrenaline 1mg/iv given. Patient developed ventricular tachycardia with a rate of 140/minute and was administered preservative free injection xylocaine 80mg/iv given. The ventricular tachycardia did not revert even after administration of additional 80 mg dose of xylocaine and progressed to ventricular fibrillation. Cardioversion done with 200Joules and CPR continued. . Cardiac activity and sinus rhythm regained. Anaesthesia was maintained with 100% O2 and Inj.Atracurium 25mg/iv. Monitored with pulseoxymetry,ECG,ETCO2,temperature and Non-invasive Blood pressures Intra-op BP were 70/40 and SPO2 90% with 100% Oxygen. Ionotropes Inj.Dopamine 20mcg/kg/min and Inj.Dobutamine 10mcg/kg/min started .Rest of the surgery was uneventful and still born baby was delivered . After the surgery, patient was shifted to Intensive Care Unit (ICU) for Ventillatory care. Patient was advised Chest X-ray and Echocardiography. X-ray chest showed cardiomegaly with a pneumonic patch in the left middle lobe of the lung but ECHO showed dilated cardiomyopathy with a severe LV dysfunction with ejection fraction of 19% ,moderate Eccentric MR. Rapid Digitalization done with inj digoxin 500mcg intravenously with in 24hours. Patient given trial extubated after 24hrs , 7 hrs after extubation ,patient developed severe respiratory distress and was again reintubated and connected to mechanical ventilator, patient completely paralysed and put on controlled ventilation. Patient was ventilated for a period of 20 days and during which she developed 2 episodes of Transient Ventricular Tachycardia, which was treated with Inj.Amiodarone 150mg given over a period of 10mins.patient underwent tracheostomy on the 11th post-op day and extubated on the 20th post-op day after the pneumonic patch has resolved and patient was doing well. CONCLUSION: Peripartum cardiomyopathy occurs in about 1 in 4000 deliveries and is often unrecognized, as symptoms of normal pregnancy commonly mimic those of mild heart failure and is usually diagnosed in the post partum period by ECHOCARDIOGRAM .Morbidity and mortality varies from 7%-50%. discharged and patient doing well We are reporting a case which was successfully managed and