Subclassified of Ovotesticular DSD
advertisement

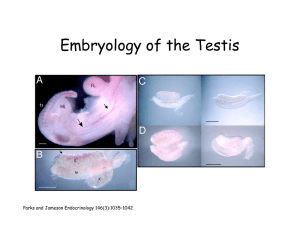
Ovotesticular Disorder of Sexual Development The diagnosis of ovotesticular DSD (true hermaphroditism)requires the presence of ovarian tissue (containing follicles) and testicular tissue in the same or the opposite gonad. Subclassified of Ovotesticular DSD - Lateral cases (20%) : A testis on one side and an ovary on the other. - Bilateral cases (30%) : Testicular and ovarian tissue present bilaterally, usually as ovotestes. - Unilateral cases (50%) : An ovotestis present on one side and an ovary or testis on the other. The ovotestis tends to be anatomically located in an ovarian position, in the labioscrotal fold, in the inguinal canal, or at the internal inguinal ring. Ovaries, when found, can occupy the normal abdominal position. Interestingly, ovaries occur more commonly on the left side than the right. The reason for this predilection is unknown. Testes are usually found in the scrotum, although they can be found at any level along the path of embryonic descent from abdomen to scrotum, frequently presenting as inguinal hernias. Ovaries and ovarian portions of ovotestes appear normal and demonstrate follicular growth with estradiol production. The presence of estradiol in developing ovarian follicles usually inhibits spermatogonia development in adjacent or contralateral seminiferous tubules. Degeneration and hyalinization of the seminiferous tubules with poor germ cell development is frequently observed. Spermatogenesis in testis and ovotestis is rare. Causes - Genetic chimerism - Nondisjunction: Postzygotic mitotic errors arising from anaphase lag may occur in 45,X/46,XY or 45,X/46,XY/47,XYY mosaicism. - X-Y translocation - Mutation: A mutation of a gene on the X chromosome or alternatively on an autosome. - Occult mosaicism. Clinical Manifestration - Vary in differentiation of the genital tract and development of secondary sex characteristics. - Most patients who present early have ambiguous genitalia or significant hypospadias. Cryptorchidism is common, but at least one gonad is palpable, usually in the labioscrotal fold or inguinal region, more often on the right, an often associated with an inguinal hernia. The differentiation of the genital ducts usually follows that of the gonad and a hemiuterus or rudimentary uterus is often present on the side of the ovary or ovotestis. - Breast development at the time of puberty is common in ovotesticular DSD. - Ovulation and pregnancy have been reported in a number of patients with a 46,XX karyotype. - Progressive androgenization. - Estrogenization at the time of puberty and may have cyclic hematuria if a uterus is present. - Spermatogenesis is rare, and interstitial fibrosis of the testis is common. Laboratory Studies - Cytogenetic investigation (peripheral karyotype, molecular studies) - Hormonal evaluation Imaging Studies - Pelvic or abdominal ultrasonography, CT scan, MRI, Genitogram, Intravenous pyelogram. Histologic Findings - Ovotestes contain both ovarian follicles and testicular tubular elements. Ovaries and ovarian portions of ovotestes appear normal. Testicular elements show degeneration and hyalinization of the seminiferous tubules with poor germ cell development. Management of ovotesticular DSD - Age at diagnosis, Genital development, Internal structures and Reproductive capacity. Gender assignment - New born : potential for normal sexual and reproductive function. - Adolescent : patient's preestablished gender Surgical Care : Conservative gonadal surgery is the procedure of choice. Medical Care : Sex hormone supplementation may be required for complete pubertal development. Prognosis - Usually do not possess other developmental malformations. - Average intelligence and have a normal life expectancy. - Female sexual assignment : Ovulation can occur, and several pregnancies have been reported. - Male sexual assignment : Spermatogenesis has been reported in only 12% of these cases. Reference - John C Achermann, Ieuan A Hughes. Disorder of Sex Development.In : Shlomo Melmed [et al.]. Williams textbook of endocrinology.12th ed. Philadelphia, PA: WB Saunders; 2011:868-891. - Sophia Ouhilal, M.D.,Jack Turco, M.D.,and Paul D. Manganiello, M.D. “ True hermaphroditism presenting as bilateral gynecomastia in an aldolescent phenotypic male”. Fertility and Sterility 2005, 83(4): 1041.e11-1041.e13. - J.W.Wit, A.O.Quartero and J.Huber. “ A phenotypic male with true hermaphroditism and a 46,XX/XY/47,XXY karyotype”. Clinical Genetic 1987: 31: 243-248.