Posterior
advertisement

حيدر.د
الزريجاوي
9/1/2014
Crossbite
C
rossbite is a discrepancy in the buccolingual
relationship of the upper and lower teeth.
Under normal circumstances the maxillary arch
overlaps the mandibular arch both labially and
buccally, i.e. the buccal cusps of the maxillary teeth are
in contact with the central fossae of the mandibular
teeth. But when the mandibular teeth, single tooth or a
segment of teeth, overlap the opposing maxillary teeth
labially or buccally, depending upon their location in
the arch, a cross bite is said to exist.
Crossbite refers to a discrepancy in transverse relationship in contrast to the
overbite which refers to vertical discrepancy. It could be associated with mandibular
displacement that means the deflection of the mandible, on closing from the rest
position into maximum interdigitation due to presence of deflecting contact(s), into
the left or right side (lateral displacement) or to the anterior (anterior displacement).
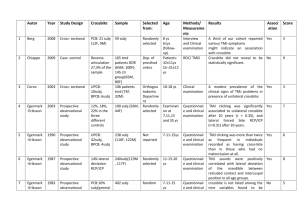
1. CLASSIFICATION:
♣Crossbite can be classified according to its location in the arch as anterior crossbite
and Posterior crossbite.
Anterior crossbite is an occlusal disorder where one or more of the upper incisors
are in linguo-occlusion (i.e. in reverse Overjet) relative to the lower arch. The
anterior crossbite may associate with anterior mandibular displacement and if so it is
known as false Anterior crossbite (i.e. pseudo CL.III).
{1}
Orthodontics.…..………...…………...…………………..…...……….Crossbite
Crossbite
Number of
Teeth
Location
Anterior
Unstable
(False)
Group
Of Teeth
Dental
Skeletal
Lingual
(Scissor)
Buccal
Stable
(True)
Single
Tooth
Posterior
Etiology
Unilateral
Bilateral
Stable
(True)
Unstable
(False)
Posterior crossbite can be classified into:
Buccal Crossbite: in which the buccal cusp of a lower tooth occlude buccal to the
buccal cusp of an opposing upper tooth. It is most common type.
Lingual Crossbite (Scissor bite): in which the buccal cusp of a lower tooth occlude
lingual to the lingual cusp of an opposing upper tooth. It is less likely type.
{2}
Orthodontics.…..………...…………...…………………..…...……….Crossbite
Posterior crossbite may be further classified according to
the existence of the cross bite on one or both sides of the
arch as Bilateral and Unilateral crossbite.
Bilateral posterior crossbites are more likely associated
with skeletal discrepancy either in the anteroposterior or
transverse dimensions, or in both.
Unilateral posterior crossbite is usually present with
lateral mandibular displacement and the common cause is
the slight narrowing of maxilla. If it so, it is called
Unstable (False) and is frequently seen in primary and
mixed dentition period. It is characterized by a midline
shift of lower arch relative to the upper arch.
Unilateral posterior crossbite without lateral mandibular
displacement is less common and usually come from
underlying skeletal asymmetry, is called Stable (True)
crossbite. It is mostly seen in adults.
♣ both anterior and posterior crossbite can be further classified according to the number of
teeth involved as Single tooth crossbite, named instanding tooth, or Segmental crossbite
which includes group of teeth.
♣ Based on the etiologic factors the crossbite can be classified as:
Dental crossbites: are generally single tooth or sometimes-segmental cross bites.
These usually result from arch length discrepancy or an abnormal path of eruption.
These are usually not accompanied by any threat to general health of the patient; the
problems arising due to such crossbites are periodontal or esthetic in nature.
{3}
Orthodontics.…..………...…………...…………………..…...……….Crossbite
Skeletal crossbites: These include those crossbites, which are primarily due to malpositioning or malformation of the jaws. This can be inherited (crossbite seen in
patients with Class III skeletal pattern), congenital (e.g. cleft lip and palate cases) or
arising due to trauma at the time of birth (e.g. unilateral ankylosis of the TMJ) or
later in life. They are capable of causing appreciable damage to a person's health
and personality as the appearance may be compromised to a larger extent.
2. AETIOLOGY:
A variety of factors acting either singly or in combination can lead to the development of a
crossbite. A good knowledge of the basic factors that cause crossbite will facilitate the
diagnosis, in turn the choosing of treatment approach.
Local Causes:
The most common local cause is lack of space (crowding) where one or two teeth are
displaced from the arch. Lack of space can come from large teeth and/or small arch, or
supernumerary teeth. For example a crossbite of an upper lateral incisor often arises
owing to lack of Space between the upper central incisor and the deciduous canine which
forces the lateral incisor to erupt palatally and in linguo-occlusion to the opposite teeth.
Posteriorly, early loss of a second deciduous molar in a crowded mouth may result in
forward movement of the first permanent molar forcing the second premolar erupt
palatally. Also, retention of primary tooth can deflect the eruption of the permanent
successor leading to crossbite.
Retention of primary molar deflect the
eruption of the permanent 2nd premolar
Lack of space cause palatal eruption of
permanent lateral incisors
Skeletal Causes:
Generally the greater the number of teeth in crossbite, the greater is the skeletal
component of the aetiology. A crossbite of the buccal segments may be due purely to:
{4}
Orthodontics.…..………...…………...…………………..…...……….Crossbite
Size discrepancy: a mismatch in the relative width of maxillary and mandibular
jaws.
Position discrepancy: an anteroposterior discrepancy, which results in a wider
part of one jaw occluding with a narrow part of the opposing jaw.
For this reason buccal crossbite of an entire buccal segment are most commonly
associated with Class III skeletal pattern, and the lingual (scissor) crossbite are
associated with Class II skeletal pattern. Anterior crossbite is associated with Class III
skeletal pattern. Crossbite can also be associated with true skeletal asymmetry.
Class III skeletal pattern
Class II skeletal pattern
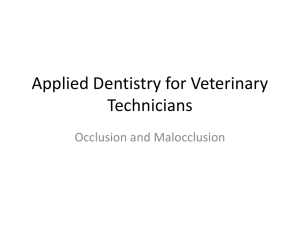
Soft Tissue and Habits:
As tongue drop down to the floor of the mouth in
bad oral habits cases (mouth breathing, adaptive
swallowing, or thumb sucking), a negative
pressure is generated intra-orally.
The reduced intra-oral pressure, possibly
combined with the activity of the buccal
musculature could produce a slight narrowing of the dental arch and production of
buccal crossbite, usually unilateral crossbite. This slight narrowing of the dental arch
leads to adopting of the lower jaw, a translocated path of closure (i.e. displacement),
and in turn development of unstable type of posterior crossbite.
{5}
Orthodontics.…..………...…………...…………………..…...……….Crossbite
Rare Causes:
They include any other factors that influence the growth of the jaws by inhibition,
changing or increasing the growth rate. For example:
Cleft lip and palate, where the growth in width of the upper jaw is restricted by
the scar tissue of the cleft repair.
Trauma to, or pathology of, TMG can lead to restriction of growth of the
mandible on one side leading to asymmetry.
3. DIAGNOSIS
Clinically:
A functional examination of the mandible’s closing pathway from maximum opening
to first contact and then final, maximum intercuspation must be performed to
determine if a lateral or anterior-posterior mandible shift occurs following first
contact.
It is important to know, how we can differentiate between skeletal crossbite (jaws'
size or position) and dental crossbite (soft tissue, habit and local causes), also
between the stable (true) and unstable (false) crossbites.
If the crossbite is anterior and posterior and bilateral so this means that it is
skeletal (as in Sk. Cl. III Malocclusion).
If the roots of molars are flared buccally with adequate palatal width, it is of
dental origin. In other words, the inter-molar distance (CD) is roughly equal or
less than the palatal width (AB).
{6}
Orthodontics.…..………...…………...…………………..…...……….Crossbite
If the palatal vault narrow and deep with teeth tilted outward more than
normal, so both palatal width (AB) and inter-molar distance (CD) are less than
normal and (CD) is considerably larger than (AB), it is mostly skeletal one.
If crossbite associated with either lateral or anterior displacement (functional
shift), it is more likely to be of dental origin.
If the unilateral posterior crossbite associated with the lower midline shifting
toward the side of crossbite, it is of unstable type.
The number of teeth involved in crossbite is a guide to the severity of the
problem with fewer involved teeth usually associated with dental type.
4. MANAGEMENT
Rationale for early treatment:
Crossbite associated with a displacement is considered as a functional indication for
early orthodontic treatment
There is some evidence that displacing contacts may predispose towards TMG
dysfunction syndrome in a susceptible individuals.
Spontaneous correction in crossbite cases is unusual even when eliminating
the etiologic factors.
If crossbite not treated early, it may result in skeletal changes, demanding a
more complex approach.
Regarding the problems that affect the maxilla-mandibular complex, the arch
width stands out because of its limited growth, as the first dimension to stop
growing.
Bilateral buccal crossbite without displacement is probably as efficient for chewing
as that the normal buccolingual relationship of teeth. However, the same cannot be
said for lingual crossbite where the cusps of affected teeth do not meet together at all.
An accurate diagnosis and treatment planning must be accomplished with the patient
in centric relation to detect the presence or absence of displacing contact. An
overcorrection expansion protocol should be applied in order to improve the
treatment stability.
Treatment Approaches:
Removal of displacing contact: In a few cases, mostly observed in the primary or
early mixed dentition, a shift into posterior crossbite will be due merely to
{7}
Orthodontics.…..………...…………...…………………..…...……….Crossbite
interference caused by the primary canines. This cause of posterior crossbite is
infrequent and is best treated by occlusal adjustment of the primary canines.
Minor canine interferences leading to
mandibular shift.
Occlusal adjustment of the primary
canines.
Removable appliances: it is indicated when the tipping tooth movement is
required for crossbite correction. Anterior crossbite due to palatally tilted
maxillary incisors, with sufficient overbite, treatment can be accomplished more
readily with a removable appliance incorporating palatal springs (like Z.& R.Z.
springs) or segmental screw for facial movement of maxillary incisors Sometimes
an active labial bow is used for lingual movement of mandibular incisors . The
appliance should have multiple clasps for good retention. Posterior biteplate to
reduce the overbite while the crossbite is being corrected usually is unnecessary
unless the overbite is exceptionally deep. A removable appliance of this type
requires nearly full -time wear to be effective and efficient.
Upper removable appliance with a midpalatal screw and buccal capping can be
used in the treatment of posterior crossbite involving all or segment of posterior
teeth, which are being tilted palatally. It mostly used in the treatment of posterior
crossbites of smaller magnitude in children and young adolescents. Also a simple
removable appliance with a T-spring can correct posterior crossbite of single
tooth like the premolars.
{8}
Orthodontics.…..………...…………...…………………..…...……….Crossbite
Fixed appliances:
A simple fixed appliance useful in the correction of
unilateral posterior crossbites consists of two banded
or bonded attachments on upper and lower teeth in
crossbite. The cross-elastic is worn full-time between
these attachments. This appliance is most effective
when the teeth in both arches contribute to the
problem and the correction requires movement of
opposing teeth in opposite direction. The vertical force
from the elastics may extrude the teeth, causing an
opening of the bite.
Banded lingual arches (W-arch and quad helix) are
Fixed appliances that expand the maxilla bilaterally
particularly at preadolescent age, producing a mix of
skeletal and dental changes. These appliances
generally deliver a few hundred grams of force and
provide slow expansion. Fixed appliances such as
these require little cooperation by the patient. For
reactivation, the W-spring and quad helix appliances
are removed from the banded teeth, widened, and
then recemented on the teeth to complete the
expansion.
Fixed maxillary expander (banded or bonded) can
be used in treatment of skeletal maxillary constriction,
through opening the midpalatal suture, up to age 15
yrs. There are two types of expansion, rapid and slow
expansion.
Rapid expansion typically is done with two turns for
screw daily (0.5 mm/day), so large force generated in
order to open the midline suture and expand the
{9}
Orthodontics.…..………...…………...…………………..…...……….Crossbite
maxilla by skeletal expansion. A diastema usually
appears between the central incisors as the bones
separate in this area.
Slow expansion is done at the rate of 1 mm/week,
so opens the suture at a rate that is close to the
maximum speed of bone formation. No midline
diastema appears, but both skeletal and dental
changes occur. The activation of screw done by one
Bonded fixed expander
turn every other day, i.e. four turns per week.
A bonded expander that covers the occlusal surface
of the posterior teeth may be a better choice for a child with a long face tendency
by producing less mandibular rotation than a banded type.
It is important to realize that heavy force and rapid expansion could be used in
late mixed and early permanent dentition to move the halves of the maxilla apart,
while it should not be used in preschool children because of the risk of producing
undesirable changes in the nose at that age.
There are several disadvantages in using of fixed expander, as it is more bulky
than expansion lingual arches and more difficult to place and remove. The patient
inevitably has problems in cleaning it, and the patient or his parent must activate
the appliance.
{10}