Autor - European Journal of Orthodontics
advertisement

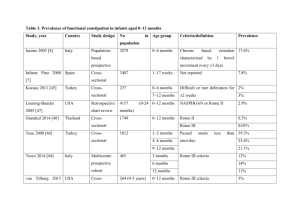
Autor Year Study Design Crossbite Sample Selected from: Age Methods/ Results Measureme nts 1 Berg 2008 Cross- sectional PCB: 21 subj (12F, 9M) 59 subj Randomly selected Interview and Clinical examination 2 Chiappe 2009 Case -control Reverse articulation 27,3% of the sample Dep. of prosthod ontics 3 Corvo 2003 Cross- sectional UPCB: 10subj, BPCB: 6subj 165 tmd patients DDR (65M, 100F); 145 ctr group(65M, 80F) 106 patients tmd (74F, 32M) 8 ys 61ys (followup) Patients: 32±11ys Ctr:31±12 ys 10-18 ys 4 Egermark -Eriksson 2003 Prospective observational study 12%, 18%, 22% in the three different controls 100 subj (56M, 44F) Orthogna todontic Departme nt Randomly selected 5 Egermark -Eriksson 1990 Prospective observational study UPCB: 42subj, BPCB: 4subj 238 subj (116F, 122M) 6 Egermark -Eriksson 1987 Prospective observational study 14% lateral deviation RCP/ICP 7 Egermark -Eriksson 1983 Prospective observational PCB:10% subj(premol Associ ation Score A third of our cohort reported Yes various TMJ-symptoms might indicate an association with crossbite Crossbite did not reveal to be No statistically significant. 3 Clinical examination A modest prevalence of the Yes clinical signs of TMJ problems in presence of unilateral crossbite. 3 Examinati on at 7,11,15 and 35 ys Questionnair e and clinical examination TMJ clicking was significantly Yes associated to unilateral crossbite after 10 years (r = 0.35), and lateral forced bite RCP/ICP (r=0.31) after 20 years. 7 Not reported 7-11-15ys Questionnair e and clinical examination 6 240subj(123M , 117F) Randomly selected 11-15-20 ys Questionnair e and clinical examination 402 subj Random 7-11-15 ys Questionnair e and clinical TMJ clicking was more than twice Yes as frequent in individuals recorded as having cross-bite than in those who had no malocclusion at all. TMJ sounds were positively Yes correlated with lateral deviation of the mandible between retruded contact and intercuspal position in all age groups. crossbite is not listed among the No nine variables found to be RDC/ TMD 9 8 5 study ar region); 9%subj(mol ar region) PCB= 157subj 8 Farella 2007 Cross- sectional 9 Helm 1984 10 Keeling 1994 Prospective observational study Cross- sectional UPCB:93sub j, BPCB:27subj PCB: 265subj 11 Marklund 2010 Prospective observational study 12 Marklund 2007 13 Miyawaki 2004 Prospective observational study Case- control UPCB (8%)subjBPCB (2%)subj UPCB and BPCB =29subj Patients with DDR and controls 14 Miyazaki 1994 Cross- sectional 15 Pahkala 2004 Prospective observational study examination associated to TMJ sound. Posterior unilateral crossbite No does not appear to be a risk factor for temporomandibular joint clicking. unilateral crossbite was Yes associated with locking of the mandible. Statistical significant association No were not detected between TMJ sounds and posterior crossbite. 7 1291 subj (708M, 583F); Schools, nonpatients Mean age 12.3±1.1 ys RDC/TMD 841subj (369M, 472F) School adult 3428 subj (52.2/47.8 male/female ratio) 280 (98M, 182F) School 6-12 ys (9±0.8) Questionnair e and clinical examination Clinical examination Dentistry students 57%<21ys 43%>21ys RDC/TMD A registered crossbite at baseline Yes was significantly related to the incidence of TMJ disorders. 9 308 subj (114M 194F) Dentistry students 23±4,9 ys(18-48) RDC/TMD 6 12 subj with DDR and 12 controls (12M, 12 F) Patients 23.8 ysand 22.9ys Radiographie s , Magnetic resonance and clinical examination PCB: 265subj 532 subj(179M 353 F) 6-38 ys Clinical examination Mean percentage in the groups 48 subj (23F, 25m); 49 ctr, (31F, 18M) Orthodon tic departme nt School for phoniatric consultati on Crossbite was with a statistically Yes significant co-morbidity to TMJ pain and/or dysfunction. Condylar movements in patients Yes with unilateral posterior crossbites might be related to the susceptibility to TMJ disc displacement, particularly the lateral portion. Posterior crossbite had a high Yes prevalence of symptoms. Examinati onat 7,10,15 e 19 ys Clinical examination Only protrusive interferences No positively related to clicking 7 2 6 6 3 PCB=7.5%su bj UPXB= 15subj 16 Pellizzoni 2006 Case-control 31 subj:15 patients (6M, 9F) and 16 control (6M, 10F) 381 patients TMD DDR and osteoarthrosis, and98 ctr (female) Patients 17 Pullinger 2000 Case-control Not reported 18 Pullinger 1993 Case- control UPCB: 73 subj 413 patients tmd, 147 ctr 19 Pullinger 1988 Cross- sectional PCB: 70subj 222 subj (102F, 120M) Student 23.9 ys mean 20 Roberts 1987 Cross- sectional 205 patients tmd (222 joints, 188 unilateral and 17 bilateral) Patients Not reported 21 Runge 1989 Cross- sectional Deflective malocclusio n: 29(same side), 30 opposite side Not reported 226 subj (103M, 123F) Dental clinic Adolesce nts and adults 22 Seligman 1989 Cross- sectional PCB= 32% ctr; 196 patients tmd, 222 ctr Dental student Not reported University students, private patients and Orofacial Pain Center Not reported Patients (9.3±2.1y s), control (9.6±2.1 ys) between 15 and 74 ys RDC/TMD Temporomandibular joint No derangement and unilateral posterior crossbite are independent occurrence. 4 Not reported Patients with disk displacement Yes were mainly characterized by unilateral posterior crossbite. Occlusal factors may be cofactors in the identification of patients with TMD, but their role should not be overstated. 9 Not reported Questionnair e and clinical examination Questionnair e and clinical examination Clinical examination and arthrography Significant increases in risk with unilateral maxillary lingual crossbite. Clicking was positive associated with unilateral posterior crossbite. Tilted teeth on the contralateral side were more common in cases of reducing meniscal dislocation than in cases of normal meniscus position or of nonreducing meniscal dislocation. No significant association between presence/absence sounds and crossbite. Yes 6 Yes 5 Yes 3 No 5 The occurrence of crossbite in No each patient diagnostic group 5 Questionnair e, stethoscope and audiovisual examination TMD patients 18% DDR; 36% DDWR UPCB: 26 subj 23 Sonnesen 2001 Case- control 24 Sonnesen 1998 Cross- sectional PCB 22.1 %subj 25 Tecco 2011 Cross- sectional 26 Thilander 2002 Cross- sectional UPCB= 45 subj BPCB= 251subj PCB: 216subj 27 Vanderas 2002 Cross- sectional PCB (46)subj, PCB with shift (17)subj (102F, 120M) 26 crossbite patients (13M, 13F); 26 ctr (13M, 13F) 104 subj (44F and 56M) 1134 subj (593M, 541F) 4724 subj (2353 F and 2371 M) 314 subj (161M, 153F) Legenda: Crossbite= number of subjects in the sample presenting crossbite PCB= posterior crossbite UPCB= unilateral posterior crossbite BPCB=bilateral posterior crossbite was similar to the control sample. Dental health service Populatio n in dental health service University patients Dental health service School 7-13 ys (patients) ; 7-13 ys (ctr) 7-13 ys Questionnair e and clinical examination Crossbite is not listed among the No variables associated to joint clicking. 4 Clinical examination There were no association No between joint sounds and malocclusion traits. 6 5-15 ys RDC/TMD Association p=.22 sound No 5 5-17 ys Questionnair e and clinical examination Stethoscope and clinical examination TMD was associated with Yes posterior crossbite; click associated to sliding. clicking and posterior crossbite No (p= 0.77); 6 6-8 ys PCB- TMJ 6 DDR= Disk Displacement with reduction DDWR=Disk Displacement without reduction RCP/ICP= retruded contact position/ intercuspal position CMD=Cranio Mandibular Disorders Subj=subjects Ctr= control group