File - Shalicia Kay J. Corson
advertisement

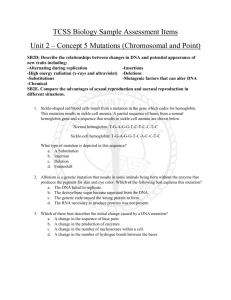
Running Head: THE EFFECTS OF THE JAK2V617F MUTATION 1 Shalicia Corson-Small The Effects of the JAK2V617F Mutation Portland State University Blood is what makes everyone tick. It courses through the veins within the body and mind like flowing river, carrying oxygen throughout the body; keeping it afloat with each pump. Evolution has taken its course through history, every now and then some slight difference, within one or two species, comes to the surface. This is known as a mutation. Mutation, by theory, has made homosapiens stand, think, and make the world what it is today. While a genetic mutation can cause change for the better, it can also revolutionize for the worse. The Janus kinase 2, more commonly known as JAK2, is a gene that provides instructions for making a certain protein that encourages the growth and division of cells. More specifically, the JAK2 protein transmits a signal from the outside of the cell to the nucleus. The JAK2 is found in every living human being on earth, but a select few with essential thrombocythemia (a disorder characterized by an increased number of platelets), resulting in large red blood cell masses. Depending on the placement of these masses, this collection of clots can cause a stroke and in some exceedingly rare cases, even death. A large red blood cell mass, or clot, is called polycythemia vera and is where we find the mutation within the JAK2; the protein that creates a fairly common mutation called Val617Phe, or for short V617F. While the JAK2 V617F blood Running Head: THE EFFECTS OF THE JAK2V617F MUTATION 2 mutation is very rare and is only found in a select few patient the alteration itself is very hard to detect, this variation within the gene is highly debated and in addition is misunderstood, the JAK2 V617F is also showing a variance within different within ethnic groups. The Janus kinase 2 is member of a family of four: Janus Kinases 1, 2, 3, and tyrosine kinase 2. Named after the Roman god of gates and passages, these non receptor kinases have both 'active' and 'inactive' domains, such as the God Janus whom had the ability to look both ways (McLornan D., 2006, p. 112). JAK2 is qualified as a Myeloproliferative disorder (MPD), a group of haematological conditions where there is "a primary disorder… leading to increased production in one or more blood cell types." (McLornan D., 2006, p. 112) Above all, this proteins job is controlling the production of blood cells from the hematopoietic stem cells. Located within the bone marrow, they will soon have the ability to become red blood cells, white blood cells, and platelets. As cited in The Narrative review: Thrombocytosis, polycythemia Vera, and JAK2 mutation: The Phonotypic Mimicry of Chronic Myeloproliferation, "the JAK2 V617F mutation is present within more than 95% of patients with polycythemia vera, and within approximately half of the patients with thrombocytosis." This makes the mutation common among patients with PV, though there is much known about this specific mutation, "the genetic basis for the disorder in patients is unknown…" (Spivak, 2010, p. 303 ). Because the basis for the mutation is unknown, Spivak makes the conclusion that if there was more knowledge about how the mutation is formed, then the patients with the JAK2 V617F would have more credible accounts of how it came to be within the body. Running Head: THE EFFECTS OF THE JAK2V617F MUTATION 3 In 1951, a man by the name of William Dameshek hypothesized that "[A] disease such as polycythemia vera, (PV), might not distinct entities but rather interrelated disorders causer by as-yet discovered stimulus acting on the bone marrow" (Spivak, 2010, p. 300). For many years his hypothesis was rejected; rejected because, at the time, Dameshek had very minimal use of resourse reguarding the findings of the JAK2 V617F mutation. But recent experiments on patients with PV, an increase in hemoglobin causing man increase in red blood cells, have shown that Dameshek may have been correct after all. Before 1989, it was impossible to detect whether a person with polycythemia vera had the JAK2V617F mutation because of an inadequacy in laboratory measurement of red blood cell mass, and schooling of the technicians (Tefferi, 2007, p. 600). Polycythemia vera, and essential thrombocytosis are unique among the myeloproliferative disorders because they both are mutation causing constitutive activation of the JAK2 (Spivak, 2010, p.301). Over all this is a outcome to Dameshek prediction. With his hypothesis being correct this changed the whole underlying perception of the JAK2 617F mutation. In discussions of Dameshek, one of the largest controversial issues has been whether or not the so-called "Dameshek theory" (Teofili, 2007, p.1049) was a legitimate hypothesis or just conjecture. On one hand, Teofili argues that at the time Dameshek did not have the proper resources to conjure up such a hypothesis. Yet, on the other hand, Spivak contends to say that, on page 303, "…Dameshek was prescient in his thinking, because the myeloproliferative disorders share many features, such as an unregulated increase in the number of circulating erythrocytes, leukocytes, or platelets, alone in combination."Spivak has more of a solid background by showing how sufficient evidence, while Teofili only states that the reason the Running Head: THE EFFECTS OF THE JAK2V617F MUTATION 4 scientific community should disreguard his theory is because she believes he did not have the proper resources. In 1978, Dameshek's hypothesis was taken legitimately and the JAK2V617F mutation was officially categorized as a myeloproliferative disorder (MPD). Myeloproliferative disorder studies have been widely discussed and have tested within a large variety of cultures. Eight hematology researchers from the Department of Hematology (the study of blood), in the All India institute of Medical Sciences in New Delhi, India, noticed that the large populations in which the JAK2 V617F mutations had mounted up to very little, there had been no studies done within an Indian culture. "Its frequency varies in different populations but there has been no data from India. We therefore, looked for JAK2 V617F mutation among Indian patients with chronic myeloproliferative disorders" (Sazawal, 2010, p.287). With this statement, the researchers went out to see if the JAK2 V617F mutation was more commonly present within the Indian culture. Screening for JAK2 V617F in patients with polycythemia vera, and essential thrombocythemia, was performed on 75 patients at the Hematology clinic in north India. Their results showed that 51 of 75 case subject had the JAK2 V617F mutation; 82 percent within the polycythemia vera patients, and 70 percent in the essential thrombocythemia subjects. When the same study was done in the United States by J. Poodt on non-Hispanic white and African American subjects as the population, Poodt gathered the results of 47 of 75 within the population had the JAK2 V617F mutation, 74 percent within the polycythemia vera patients, and 71 percent within the essential thrombocythemia (Poodt,2006 p.230) . With the collected Running Head: THE EFFECTS OF THE JAK2V617F MUTATION 5 results, a statistician could gather that inside the data given, the mutation is more strongly represented with the Indian community. The JAK2 V617F variation is very rare and deadly. While much is known about it today, "the janus kinases 2 mutation, is becoming incredibly unreported among patients that are healthy and do not know that they have a myeloproliferative disorder" (Benos D., 2012, p. 300). If the screening was available to the public, and understood by hematologists, then Spivak says "possibly 25% of patients deaths could be prevented" (2010 p.304). In addition, the mutation is proven to be more present in ethnic cultures (Poodt, 2010). "Mutation is the ultimate source of all genetic variation found in natural populations and the only new material available for natural selection to work on" (Mayr E., Populations, Species, & Evolution, 1970, p.102). If more funding and awareness of this mutation were known where would the JAK2 V617F mutation be today? Running Head: THE EFFECTS OF THE JAK2V617F MUTATION 6 Reference Page Mayr E. Populations, species, and evolution. April 1970 McLornan D., Percy M., & McMullin M. F. (2006). JAK2 V617F: a single mutation in the myeloproliferative group of disorders. The Ulster medical journal, 75(2), 112-119. Poodt J., Fijnheer R., Walsh IBB., Hermans MHA. A sensitive reliable semi-quantitative real-time PCR assay to detect JAK2 V617F in blood, Hematol. Oncol. September 2006; 24: 227233, DOI: 10.1002/hon.800 Sazawal S., Bajaj J., Chikkara S., Jain S., Bhargava R., Mahapatra M., & Saxena R. (2010). Prevalence of JAK2 V617F mutation in Indian patients with chronic myeloproliferative disorders. Spivak J. Narrative Review: Thrombocytosis, polycythemia vera, and the JAK2 mutations: the phenotypic mimicry of chronic myeloproliferation, Ann Intern Med. March 2010; 152:300-306 Vol. 152 Tefferi A., Pardanani A. Evaluation of "increased" hemoglobin in the JAK2 mutations era: a diagnostic algorithm based on genetic tests, Mayo Clin Proc. May 2007; 82(5):599-604 Teofili L., Giona F., Martini M., Cenci T., Guidi F., Torti L., Palumbo G., Amendola A., Foa R., Larocca L. Markers of myelproliferative diseases in childhood polycythemia vera and Running Head: THE EFFECTS OF THE JAK2V617F MUTATION essential thrombocythemia, J Clin Oncol. December 2013; 25: 1048-1053, DOI: 10.1200/JCO.2006.08.6884 7