mmr vaccine and autism - Association of American Colleges
advertisement

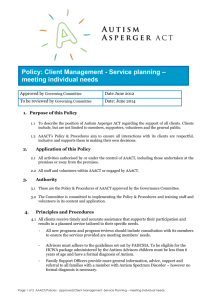
STUDENT CASE STUDY, PART TWO B: COHORT STUDY—SINGER-FREEMAN MMR VACCINE AND AUTISM: SCIENTIFIC INQUIRY, ETHICS, AND EVIDENCEBASED PROBLEM SOLVING CASE STUDY FOR THE AACU STIRS PROGRAM Karen Singer-Freeman, Associate Professor of Psychology, Purchase College, State University of New York STUDENT CASE Part Two B: Cohort Study How Can We Study the Effects of Potentially Dangerous Treatments? Methods Used in the Study of Vaccines and Autism Cohort Study When we examine naturally occurring differences in a population followed over time, we are using a cohort study. We know that some parents decide not to vaccinate their children, while most do. We could therefore compare autism rates between these two groups of children. Cohort studies are useful because they allow us to study the effects of potentially dangerous experiences without creating this danger in order to conduct the study. However, in a cohort study we always must be careful about drawing causal conclusions. Because we did not randomly assign subjects to groups there may be other differences between the groups that cause the differences we believe to be resulting from our exposure (in this case, the MMR vaccination). For example, if we wished to know whether smoking causes heart disease it would be unethical to randomly assign a group of people to start smoking (because we know that smoking causes cancer). However, if we compare the heart health of an existing group of smokers to an existing group of non-smokers there might be other differences between the groups that contribute to heart health. For example, non-smokers might be more likely to exercise, get enough sleep, or eat healthy food than smokers. Figure 9 summarizes the important features of Cohort Study design. Population of All Children Vaccinated Children Measure Autism Rates Unvaccinated Children Measure Autism Rates Figure 1. Cohort Study Design to Examine the Association between the MMR Vaccine and Autism. STUDENT CASE STUDY, PART TWO B: COHORT STUDY—SINGER-FREEMAN A Real Cohort Study Madsen et al. (2002) completed a cohort study by examining the medical records of all Danish children born between 1991 and 1998. Of the 537,303 children in this study, approximately 82 percent received the MMR vaccine. Vaccination was not associated with increased risk of autism. Among the children who had autism, there was no association between the development of their symptoms and their receipt of the vaccination. Key Questions 28) How might unvaccinated children (and families) differ from vaccinated children (and families)? Describe at least two ways these children could differ. 29) How could the differences you identified in your answer to question 28 influence the prevalence of autism in children in each group? One reason that people believed that the MMR vaccine caused autism is that this vaccine is given shortly after the first birthday. Many children begin to display the first symptoms of autism at around this time (Offit and Coffin 2003). Human beings have many cognitive biases that affect the way they think about information. One of these is the confirmation bias. The confirmation bias causes us to pay attention to evidence that supports our beliefs and be less likely to notice information that disproves our beliefs (Stanovich, West, and Toplak 2013). Let’s think about the way this might influence parents’ perception of vaccines and autism. Look at tables below, which summarize the data from the Madsen et al. 2002 study. If we believe that the MMR vaccine causes autism, the confirmation bias might cause us to pay more attention to children with autism who received the MMR vaccine and those without autism who were unvaccinated (highlighted cells), ignoring the many disconfirming cases of individuals who received the MMR vaccine and did not develop autism and those who developed autism despite not being given the MMR vaccine. These numbers could reinforce our belief that the MMR vaccine causes autism. Tables Summarizing Data from Madsen et al. 2002 MMR Vaccine Autism No Autism Vaccinated Children A 269 Children 0.11% B STUDENT CASE STUDY, PART TWO B: COHORT STUDY—SINGER-FREEMAN Unvaccinated Children C D 96,601 Children 99.95% However, if the MMR vaccine actually caused autism it should influence the incidence of autism so that the proportion of children with autism will be higher in the population of children who received the MMR vaccine than in the population of children who did not receive the MMR vaccine. An observational study that uses a cohort design (such as the one conducted by Madsen et al. 2002) provides us with data for all four of the squares above (A, B, C, D). In this way, a cohort study can help us to see whether children who are unvaccinated are more or less likely to develop autism than those who are vaccinated. The data from Madsen’s study show similarly small proportions of children developed autism in both groups. The percentage of vaccinated children who developed autism (.11%) was not significantly different (p < .05) than the percentage of unvaccinated children who developed autism (.05%). MMR Vaccine Autism No Autism 240,655 Vaccinated Children A B 269 Children 240,386 0.11% Children 99.89% 96,648 Unvaccinated Children C D 47 Children 96,601 0.05% Children 99.95% STUDENT CASE STUDY, PART TWO B: COHORT STUDY—SINGER-FREEMAN Key Questions 30) Explain how a cohort study allows you to avoid being fooled by the confirmation bias. 31) Explain why Madsen et al. (2002) did not conclude that the MMR vaccine causes autism even though more vaccinated children developed autism than unvaccinated children. 32) Propose another way to study the relation between the MMR vaccine and the development of autism. Be sure to include the group or groups you would study, the information you would gather, and how this study would add to our understanding of vaccine safety. Once your group is done with these questions, please see your instructor for guidance on next steps.