In 45 patients, the UTI was ascribed to E. faecalis. The
advertisement

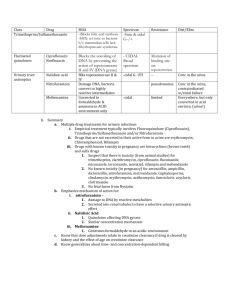
Wide consultation on fluoroquinolone MIC breakpoints for Enterococcus spp. from urinary tract infections This consultation concerns the proposal for fluoroquinolone breakpoints for enterococci from UTI only. As a result of intrinsic and acquired resistance, treatment options for enterococcal urinary tract infections (UTI) are limited. EUCAST has defined quinolones as inappropriate for treatment of systemic infections caused by enterococci and currently has no breakpoints for the use of fluoroquinolones for treatment of enterococcal UTI. Clinical data on treatment of UTI with fluoroquinolones are sparse and relate almost exclusively to Enterococcus faecalis. It is proposed that breakpoints for ciprofloxacin and levofloxacin for UTI are based on epidemiological cut-off values (ECOFFs). A review of background data is provided below. MIC distributions for Enterococcus faecalis MIC (mg/L) Agent ≤0.016 0.03 0.06 0.12 0.25 0.5 1 Ciprofloxacin 2 9 3 17 76 679 Levofloxacin 0 1 0 32 35 464 2 4 2094 631 2999 1551 32 64 ≥128 ECOFF 231 341 562 446 4 117 1205* 44 192 4 8 16 120 53 134 1065* *Includes truncated distributions MIC distributions for Enterococcus faecium MIC (mg/L) Agent ≤0.016 0.03 0.06 0.12 0.25 0.5 1 2 4 8 16 32 64 ≥128 ECOFF Ciprofloxacin 0 0 0 4 124 572 923 919 786 165 23 56 162 278 4 Levofloxacin 0 0 0 7 6 43 123 288 97 41 105 216* 107 40 4 *Includes truncated distributions Proposed fluoroquinolone clinical breakpoints for Enterococcus spp. from UTI Antimicrobial agent Ciprofloxacin Levofloxacin Clinical breakpoint for urinary tract infections S≤ (mg/L) 4 4 R> (mg/L) 4 4 Comments Comments on the proposed clinical breakpoints, together with supporting documentation if appropriate, should be sent before 14 June 2013 to the EUCAST Scientific Secretary (derek.brown222@btinternet.com). Consultation on fluoroquinolone breakpoints for Enterococcus spp. from UTI 25 March 2013 Is there a role for the fluoroquinolones in the treatment of enterococcal urinary tract infections? - a review of pre-clinical and clinical data. Oskar Ekelund and Gunnar Kahlmeter Department of Clinical Microbiology, Växjö County Hospital, Sweden Introduction Enterococci are commensals of the human gastrointestinal tract and are as such frequently isolated from clinical specimens in the clinical microbiology laboratory. While endocarditis and blood stream infections are the most severe manifestations associated with enterococci, they are in the clinical setting more often associated with urinary tract infections (UTIs) and sometimes soft tissue infections. Possibly partly due to their intrinsic decreased sensitivity or resistance to many empirically used antibiotic regimens (carbapenems, cephalosporins, aminoglycosides), enterococci are a common finding in nosocomial infections. Ampicillin has long been the mainstay in the treatment of enterococcal infections, although Enterococcus faecium is now almost always resistant to aminopenicillins. Alternative regimens include vancomycin and linezolid. Trimethoprim, with or without sulfamethoxazole, has been used in the treatment of enterococcal UTI but its efficacy in these situations has been questioned due to the ability of enterococci to incorporate exogenous folate, thereby by-passing the mechanism of action of trimethoprim (Tegmark Wisell, et al., 2008). Effective oral regimens are thus scarce and may in the case of intolerance to beta-lactam antibiotics even be lacking. Opening up a new class of drugs for the treatment of enterococci would be clinically very useful. Fluoroquinolones are due to their efficacy, tolerability and their availability as oral regimens frequently used in the treatment of complicated UTI (cUTI) and acute pyelonephritis (AP). EUCAST has deemed quinolones inappropriate for enterococcal systemic infections but so far not evaluated the use of quinolones for enterococcal UTI. CLSI has issued clinical breakpoints for four different quinolones, applicable also for the treatment of systemic infections (table 1). The role of fluoroquinolones in the treatment of enterococcal UTI will be reviewed here. Modes of action The main targets of quinolones are DNA gyrase and topoisomerase IV which are encoded by the gyrA/gyrB and parC/parE genes respectively. These enzymes have essential roles in DNA replication by catalyzing supercoiling and decatenation of DNA. The quinolones act by binding to a complex of each of these enzymes and DNA and the resulting complexes, including the drug, block the process of DNA replication (Drlica & Zhao, 1997). In gramnegative bacteria DNA gyrase is the primary target of quinolones, whereas topoisomerase IV seems to be of greater importance in gram-positives such as Staphylococcus aureus (Ferrero, et al., 1994). For enterococci the relative importance of the two proteins are unclear and affinity may be varying between different quinolones (Oyamada, et al., 2006). Intrinsic activity The MIC distributions for relevant fluoroquinolones are shown in Figures 1 – 4. The ECOFFs for enterococci are higher than those for most gram-negative bacteria (table 2). A possible explanation for this intrinsically reduced activity of quinolones against enterococci may be the presence of a chromosomal gene, qnrE.faecalis, which exhibits considerable homology with the plasmid-borne qnr sometimes found in gram-negatives. In Enterobacteriacae, qnr encodes a Consultation on fluoroquinolone breakpoints for Enterococcus spp. from UTI 25 March 2013 protein which protects DNA gyrase against the action of quinolones and inactivation of qnrE.faecalis in enterococci has in fact been shown to result in two-fold reductions in the MICs of ciprofloxacin (Arsène & Leclercq, 2007). A lower affinity of enterococcal DNA gyrase for quinolones may also theoretically be a reason for the relative intrinsic resistance. As for other gram-positive bacteria, moxifloxacin stands out as the quinolone with the lowest MIC values for enterococci. Acquired resistance In Enterococcus faecalis amino acid substitutions in the quinolone resistance-determining regions (QRDR) of gyrA/gyrB and parC/parE have been shown to be associated with quinolone resistance (Oyamada, et al., 2006). Single nucleotide substitutions in parC seem to have quite a modest effect on the MIC while simultaneous alterations in gyrA result in high-level resistance (Kanematsu, et al., 1998). Similar findings have been made in E. faecium. Furthermore, there are strains of both species carrying multi-drug efflux pumps with a consequent decrease in intracellular accumulation of quinolones (Oyamada, et al., 2006). Activity of quinolones in urine Urine is in many ways a different environment than tissues, blood and extracellular fluid. The pH is generally lower and the content of proteins and electrolytes differs from most body compartments and from that of broth used for susceptibility testing. This may affect the activity of certain antibiotics. One example is the activity of aminoglycosides (particularly against pseudomonas) which is clearly dependent on the concentration of magnesium (Mg) and calcium (Ca) (Kenny, et al., 1980). The antibacterial activity of quinolones is also affected by both pH and the presence of cations. The pH in urine normally varies between 4.4 and 8.0 and the activity of most quinolones is reduced in acidic environments. Also, high levels of magnesium (as in urine) increase the MIC values of pathogens normally susceptible to quinolones (Smith & Ratcliffe, 1986). The minimum bactericidal concentrations (MBC) in urine for most bacteria, including enterococci, are significantly higher than their corresponding MBCs of quinolones in broth (Well, et al., 1998). The degree of renal excretion, and thus the concentration, is variable between different quinolones (table 3). After ingestion of 400 mg of moxifloxacin only approximately 20% of the parent compound will be recovered in urine, whereas the renal excretion of both ciprofloxacin and levofloxacin are significantly higher. Moxifloxacin is for this reason not approved for the treatment of UTI and despite the low MIC values for enterococci, the low renal clearance of the compound probably limits its utility also in the treatment of enterococcal UTI. Altogether, neither the MICs of bacteria, nor the accepted Pk/Pd breakpoints of quinolones are automatically applicable to UTI. Furthermore, enterococci are well known producers of biofilms. In a study of 352 E. faecalis strains recovered from patients with complicated UTI, a majority of them exhibited strong or medium biofilm formation (Seno, et al., 2005). In biofilms the susceptibility of enterococci to many antibiotics, including quinolones, is decreased with minimum biofilm eradication concentrations many times higher than the MIC of the strain (Holmberg, et al., 2012). Pk/Pd studies In order to compare the efficacy of different quinolones and to take into account some of the above mentioned factors affecting the antibacterial effect of quinolones in urine, studies of urinary bactericidal titers (UBT) have been undertaken. The UBTs of an antibiotic is determined by collecting urine at specified intervals after ingestion of a dose of the compound. Urine from each interval is then diluted with antibiotic-free urine from the same individual, in doubling dilutions from 1:1, 1:2, 1:4 etc to 1:1024. The bacterial strain of interest is then added and the UBT is defined as the highest dilution step that shows antibactericidal activity. Consultation on fluoroquinolone breakpoints for Enterococcus spp. from UTI 25 March 2013 When comparing a single dose of 500mg ciprofloxacin to 400mg enoxacin or 400mg norfloxacin, ciprofloxacin exhibits superior UBTs compared to the other two quinolones, with bactericidal titres for enterococci remaining for up to 24 hours after administration of the drug (Well, et al., 1998). Levofloxacin 500mg, in turn, results in higher UBTs compared to ciprofloxacin 500mg regardless of the lower MIC values of the latter in gram-negative bacteria. When looking at gram-positives such as E. faecalis the difference is even more pronounced suggesting that levofloxacin 500mg q.d. might be superior to ciprofloxacin 500mg b.i.d. for the treatment of enterococcal UTI (Naber, 2001; Wagenlehner, et al., 2006). Levofloxacin and ciprofloxacin therefore theoretically constitute the most effective quinolone compounds for the treatment of enterococcal UTI currently under consideration. Clinical studies In order to assess the clinical usefulness of quinolones in the treatment of enterococcal UTI a literature search was performed. Studies were selected on the basis of these criteria: clinical trials of cUTI and/or AP in which ciprofloxacin and/or levofloxacin was evaluated for microbiological eradication and/or clinical cure; doses used being those recommended for cUTI and AP, i.e. minimum daily doses of 1000mg and 500mg for ciprofloxacin and levofloxacin respectively; studies containing at least ten subjects with either E. faecalis or E. faecium as the causative agent, the two species reported separately. Studies of prophylactic treatment or sequential treatment with non-quinolone antibiotics were excluded, as were nonEnglish language articles. Using the criteria above, we found no more than three clinical trials of quinolone treatment of cUTI/AP which had included at least ten patients with infections due to E. faecalis (table 4). We were not able to find any study with ten or more patients with UTI due to E. faecium. Talan (Talan, et al., 2004) 435 patients with cUTI or AP were evaluated for microbiological eradication and clinical cure after treatment with ciprofloxacin 1000mg daily for 7 to 14 days, administered either as 500mg b.i.d. or using an extended-release formulation (XR) 1000mg once daily. A majority of the patients had cUTI while only a minor part had AP. Patients with uropathogens with a ciprofloxacin MIC above 2 mg/L were excluded. In 45 patients, the UTI was ascribed to E. faecalis. The microbiological eradication rate among these was 80% at end of treatment visit, compared to the overall 94% regardless of uropathogen. Peterson (Peterson, et al., 2008) 1109 patients with cUTI or AP were evaluated for microbiological eradication and clinical cure using either levofloxacin 750mg q.d. for 5 days or ciprofloxacin 500mg b.i.d. for 10 days. The larger part of the study population had cUTI. Subjects were excluded if they prior to enrollment had pathogens known to be resistant to the study drugs. Subjects whose study entry uropathogens were resistant to any of the study drugs could remain in the study provided they were clinically stable. In 37 patients, the UTI was ascribed to E. faecalis. 12 of 16 (75%) in the ciprofloxacin-treated subjects had microbiological eradication at end of treatment evaluation. In the levofloxacin group the corresponding figure was 13 of 21 (62%). Of the 8 treatment failures in the levofloxacin group 3 consisted of highly quinolone-resistant strains. If these are excluded the eradication rate rises to 72%. Eradication rates for all pathogens were 79.8% and 77.5% in the levofloxacin and ciprofloxacin group, respectively. Naber (Naber, et al., 2004) 1123 subjects with cUTI or AP were evaluated for microbiological eradication and clinical cure after treatment with either gatifloxacin 200mg or 400mg or ciprofloxacin 500mg b.i.d. for Consultation on fluoroquinolone breakpoints for Enterococcus spp. from UTI 25 March 2013 5 to 14 days. 70% of the study population consisted of subjects with cUTI. Subjects were excluded if the uropathogen exhibited resistance to the study drugs prior to study inclusion. After enrollment, patients with uropathogens classified as resistant (MIC >2 mg/L) could remain in the study provided clinical improvement was seen. In 29 patients in the ciprofloxacin group, the UTI was ascribed to E .faecalis. Of these 23 (79%) showed microbiological eradication at end of treatment visit. Eradication rates for all pathogens were 85% in the ciprofloxacin group. Summary There is a need to add to the arsenal of antibiotics for use in the treatment of UTI caused by enterococci. MIC and pk/pd studies suggest that levofloxacin and ciprofloxacin probably are the most potent compounds in the fluoroquinolone group for this purpose. There is a lack of clinical trials addressing this issue. Also, the absence of a non-quinolone comparator compound complicates the assessment of the observed cure rates. Performing a literature search for ampicillin/amoxicillin using the same criteria as described for quinolones, we were not able to find any clinical studies fulfilling the criteria. Based on this we conclude that the use of amoxicillin/ampicillin in the treatment of cUTI due to enterococci is based on tradition rather than clinical evidence. The cure rates using these compounds are thus not known. Nevertheless, the few studies where the efficacy of quinolones was addressed indicate that a majority of subjects with cUTI or AP due to E. faecalis achieve microbiological eradication when treated with levofloxacin or ciprofloxacin. The corresponding data for E. faecium are too scarce to permit conclusions. In summary, we find there is some data supporting the issuing of clinical breakpoints for levofloxacin and ciprofloxacin for the treatment of cUTI and AP caused by E. faecalis but not by E. faecium. In the absence of studies to support a higher clinical breakpoint, the ECOFF should be used. The breakpoint could be accompanied by a caveat regarding the relatively scarce clinical data. References Arsène, S. & Leclercq, R., 2007. Role of a qnr-Like Gene in the Intrinsic Resistance of Enterococcus faecalis to Fluoroquinolones. Antimicrobial Agents and Chemotherapy, 51(9), pp. 3254-3258. Barman Balfour, J. & Wiseman, L., 1999. Moxifloxacin. Drugs, 57(3), pp. 363-373. Brittain, D. o.a., 1985. The pharmacokinetics and serum and urine bactericidal activity of ciprofloxacin. Journal of Clinical Pharmacology, Volym 25, pp. 82-88. Chien, S., Chow, A., Natarajan, J. & Williams, R., 1997. Absence of Age and Gender Effects on the Pharmacokinetics of a Single 500-Milligram Oral Dose of Levofloxacin in Healthy Subjects. Antimicrobial Agents and Chemotherapy, 41(7), pp. 1562-1565. Drlica, K. & Zhao, X., 1997. DNA Gyrase, Topoisomerase IV, and the 4-Quinolones. Microbiology and Molecular Biology Reviews, 61(3), pp. 377-392. EUCAST, 2012. Online] Available at: http://www.eucast.org [Last accessed 22 August, 2012]. Ferrero, L. o.a., 1994. Cloning and primary structure of Staphylococcus aureus DNA topoisomerase IV: a primary target of fluoroquinolones. Mol Microbiol, Volym 13, pp. 641-653. Holmberg, A., Mörgelin, M. & Rasmussen, M., 2012. Effectiveness of ciprofloxacin or linezolid in combination with rifampicin against Enterococcus faecalis in biofilms. Journal of Antimicrobial Chemotherapy, Volym 67, pp. 433-439. Kanematsu, E. o.a., 1998. Alterations in the GyrA subunit of DNA gyrase and the ParC subunit of DNA topoisomerase IV associated with quinolone resistance in Entercoccus faecalis.. Antimicrob Agents Chemother, Volym 42, pp. 433-435. Kenny, M. o.a., 1980. Cation Components of Mueller-Hinton Agar Affecting Testing of Pseudomonas aeruginosa Susceptibility to Gentamycin. Antimicrobial Agents and Chemotherapy, 17(1), pp. 55-62. Naber, K., 1997. Antibacterial activity of antibacterial agents in urine: an overview of applied methods. i: T. Bergan, red. Urinary Tract Infections and Infectiology. Basel: Karger, pp. 74-83. Naber, K., 2001. Which fluoroquinolones are suitable for the treatment of urinary tract infections?. International Journal of Antimicrobial Agents, Volym 17, pp. 331-341. Consultation on fluoroquinolone breakpoints for Enterococcus spp. from UTI 25 March 2013 Naber, K. o.a., 2004. Gatifloxacin 200 mg or 400 mg once daily is as effective as ciprofloxacin 500 mg twice daily for the treatment of patients with acute pyelonephritis or complicated urinary tract infections. International Journal of Antimicrobial Agents, Volym 23S, pp. S41-S53. Oyamada, Y. (., Ito, H. & Inoue, M., 2006. Topoisomerase mutations and efflux are associated with fluoroquinolone resistance in Enterococcus faecalis. Journal of Medical Microbiology, Volym 55, pp. 1395-1401. Oyamada, Y. o.a., 2006. Combination of known and unknown mechanisms confers high-level resistance to fluoroquinolones in Enterococcus faecium. J Med Microbiol, Volym 55, pp. 729-736. Peterson, J. o.a., 2008. A double-blind, randomized comparison of levofloxacin 750 mg once-daily for five days with ciprofloxacin 400/500 mg twice-daily for 10 days for the treatment of complicated urinary tract infections and acute pyelonephritis.. Urology, Volym 71, pp. 17-22. Seno, Y. o.a., 2005. Clinical Implications of Biofilm Formation by Enterococcus faecalis in the Urinary Tract. Acta Medica Okayama, 59(3), pp. 79-87. Smith, J. & Ratcliffe, N., 1986. Einfluss von pH-Wert und Magnesium auf die antibakterielle Aktivität von Chinolonpreparaten. Infection, 14(Suppl 1), pp. S31-S35. Talan, D. A. o.a., 2004. Once daily, extended release ciprofloxacin for complicated urinary tract infections and acute uncomplicated pyelonephritis. The Journal of Urology, Volym 171, pp. 734-739. Tegmark Wisell, K., G, K. & CG, G., 2008. Trimethoprim and enterococci in urinary tract infections: new. Journal of Antimicrobial Chemotherapy, Volym 62, pp. 35-40. Wagenlehner, F. o.a., 2006. Concentrations in plasma, urinary excretion and bactericidal activity of levofloxacin (500 mg) versus ciprofloxacin (500 mg) in healthy volunteers receiving a single oral dose.. International Journal of Antimicrobial Agents, Volym 28, pp. 551-559. Well, M., Naber, K., Kinzig-Schippers, M. & Sörgel, F., 1998. Urinary bactericidal activity and pharmacokinetics of enoxacin versus norfloxacin and ciprofloxacin in healthy volunteers after a single oral dose. International Journal of Antimicrobial Agents, Volym 10, pp. 31-38. Consultation on fluoroquinolone breakpoints for Enterococcus spp. from UTI 25 March 2013 Table 1. CLSI quinolone breakpoints for enterococci (CLSI, 2012). MIC (mg/L) Agent S≤ R> Remarks Ciprofloxacin 1 2 Levofloxacin 2 4 Norfloxacin 4 8 Gatifloxacin 2 4 Apply to UTI isolates only Table 2. Quinolone epidemiological cut-off values (ECOFFs) for enterococci and five other species (EUCAST, 2012). MIC (mg/L) Ciprofloxacin Levofloxacin Moxifloxacin Norfloxacin E. faecalis 4 4 1 8 E. faecium 4 4 1 nd E. coli P. aeruginosa S.aureus S. pyogenes S. pneumoniae nd = no data 0.064 0.5 1 1 2 0.25 2 1 2 2 0.25 4 0.25 0.5 0.5 0.25 2 4 nd 16 Table 3. Renal excretion of quinolones after intake of a single oral dose. Compound Dose Amount of parent drug Source excreted in urine Levofloxacin 500mg 76% Chien, et al., 1997 Ciprofloxacin 500mg 43% Brittain, et al., 1985 Moxifloxacin 400mg 20% Barman Balfour & Wiseman, 1999 Norfloxacin 400mg 22% Well, et al., 1998 Table 4. Clinical studies of UTI treatment using quinolones where a minimum of ten patients with infection due to E.faecalis are included (Talan, et al., 2004; Peterson, et al., 2008; Naber, et al., 2004) Author Antibiotic Daily dose Eradication rate E.faecalis Talan Ciprofloxacin 1000mg 36/45 (80%) Eradication, all pathogens 94% Cip-BID 19/27 (70%) 93% Cip-XR 17/18 (94%) 95% Peterson Naber MIC (mg/L) exclusion MIC >2 Indwelling catheters included Yes Ciprofloxacin 1000mg 12/16 (75%) 78% No** Yes Levofloxacin 750mg 13/21 (62%)* 80% No** Yes Ciprofloxacin 1000mg 23/29 (79%) 85% No*** No * 13/18 (72%) if isolates with MIC > 32 are excluded ** Subjects with resistant isolates could remain in the study if they were clinically stable *** Subjects with resistant isolates could remain in the study if clinical improvement was seen Cip-BID = ciprofloxacin 500mg b.i.d. Cip-XR = ciprofloxacin 1000mg extended-release formulation q.d. n.r.s. = not reported separately for each species Consultation on fluoroquinolone breakpoints for Enterococcus spp. from UTI 25 March 2013 Figure 1. MIC distribution of ciprofloxacin for E. faecalis (EUCAST, 2012). Figure 2. MIC distribution of levofloxacin for E. faecalis (EUCAST, 2012). Consultation on fluoroquinolone breakpoints for Enterococcus spp. from UTI 25 March 2013 Figure 3. MIC distribution of moxifloxacin for E. faecalis (EUCAST, 2012). Figure 4. MIC distribution of norfloxacin for E. faecalis (EUCAST, 2012). Consultation on fluoroquinolone breakpoints for Enterococcus spp. from UTI 25 March 2013