Rudimentary Uterine Horn presenting as a Tubal Mass
advertisement

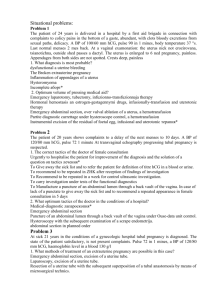
Rudimentary Uterine Horn Presenting as a Tubal Mass A Papneja1*, BSc, MD Candidate 2014 & A Murji2, MD 1 2 University of Toronto Department of Obstetrics and Gynecology, University of Toronto *anjali.papneja@utoronto.ca A 33-year-old nulligravida woman was referred for an incidental ultrasound finding of a 1 x 3 cm solid mass with increased vascularity in the right fallopian tube. The patient was asymptomatic. Physical exam revealed unremarkable external genitalia, normal cervix and non-tender, mobile, right adnexal mass. The differential diagnosis at this point included: ectopic pregnancy, fibroid, tubal carcinoma, mullerian anomaly. To rule out an ectopic pregnancy, Beta-HCG was ordered and was subsequently negative. MRI demonstrated a 2.3 x 1.6 cm solid mass in the infundibular/ampullar portion of the right fallopian tube (Figure 1, arrow) consistent with either tubal leiomyoma or carcinoma. Laparoscopy (Figure 2) revealed a unicornuate uterus (U) with non-communicating right uterine horn (arrow), normal bilateral ovaries and tubes. Subsequently, renal ultrasound was obtained and was normal. No further treatment was offered. The patient was advised to have an early ultrasound in the event of pregnancy due to the literature reporting ectopic pregnancies in non-communicating rudimentary horns. [1] Female embryological development is dictated by the absence of a Y chromosome. The SRY gene on the Y chromosome codes for Testis Determining Factor and in its absence the undifferentiated gonads become ovaries. With insufficient levels of testosterone, the Wolffian (mesonephric) ducts regress, while the Mullerian (paramesonephric) ducts continue to develop. As the Mullerian ducts migrate caudally toward the urogenital sinus, the two inferior ends fuse to form the uterovaginal canal [2]. The uterovaginal canal further differentiates into the uterus, cervix and upper portion of the vagina (Figure 3). Mullerian anomalies generally result from either a defect in Mullerian agenesis or an error in fusion of the Mullerian ducts. Our patient has a unicornuate uterus with a rudimentary horn, which is the result of abnormal development of one of the two Mullerian ducts. Approximately two-thirds of all unicornuate uteri occur with a rudimentary horn, indicating partial development of the contralateral Mullerian system. Approximately half of such non-communicating rudimentary horns contain functioning endometrium (Figure 4) and commonly present in adolescence with progressive dysmenorrhea. Ectopic pregnancy in rudimentary horns has also been described and occurs due to trans-peritoneal embryo migration [3]. A unicornuate uterus poses certain reproductive risks including, recurrent pregnancy loss, preterm labor and delivery, intrauterine fetal growth restriction and abnormal presentation. Finally, women with Mullerian anomalies have a strong association with renal anomalies (renal agenesis, pelvic or horseshoe kidney) and must be investigated appropriately [5]. Key Learning Points: Ectopic pregnancy must be ruled out women of reproductive age presenting with a pelvic mass. A unicornuate uterus results from a failure of one Mullerian duct to develop or elongate. Women with a unicornuate uterus is at risk for: obstructed rudimentary horn, ectopic pregnancy and adverse pregnancy outcomes, Mullerian anomalies have a 30% association with renal anomalies necessitating ultrasound investigation. References [1] Jayasinghe Y, Rane A, Stalewski H, Grover S. The Presentation and Early Diagnosis of the Rudimentary Uterine Horn. Obstet Gynecol 2005; 105(6):1456-67. [2] Emans, S. Jean Herriot; Laufer, Marc R.; Goldstein, Donald P. 2005. Pediatric and Adolescent Gynecology. Philadelphia: Lippincott Williams & Wilkins. [3] Shulman, Lee P. Mullerian Anomalies. Clinical Obstetrics and Gynecology 2008; 51(1):214-22 [4] The American Fertility Society classifications of adnexal adhesions, distal tubal obstruction, tubal occlusion secondary to tubal ligation, tubal pregnancies, mullerian anomalies and intrauterine adhesions. Fertil Steril 1988; 49:944-95 [5] Li S, Alya Quayyum FV, Hricak Cand H. Journal of Computer Assisted Tomography. 2000;24:829-834 Figures Consent to publish these images was obtained from the patient. U Figure 1: MRI image demonstrating a 2.3 x 1.6 cm solid mass in the infundibular/ampullar portion of the right fallopian tube. Figure 2: Laparoscopic image revealing unicornuate uterus (U) with non-communicating right uterine horn (arrow), normal bilateral ovaries and tubes. Figure 3: Embryological development of the female genital tract. [2] Figure 4: Anatomical and functional variations of a unicornuate uterus anomaly. [4]