Ectopic Pregnancy
advertisement

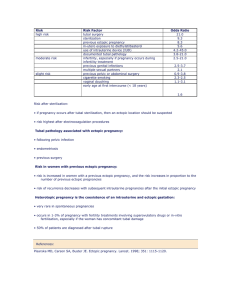
ECTOPIC PREGNANCY Dr.Najwa.B.Eljabu Arab & Libyan Board Msc reproductive and Maternal sciences Glasgow University DEFINITION Ectopic pregnancy is implantation occurring outside the uterine cavity. Either implanted outside the uterus (fallopian tube, ovary and abdominal cavity) or in abnormal position within the uterus (cornua, cervix). Combined tubal and uterine (Heterotopic) pregnancies are uncommon) It is a major cause of maternal mortality in the first trimester. OVERVIEW Incidence Increasing (16/1000 Pregnancies in UK) 95-98% tubal 50% ampulla 20% isthmus 12% fimbrial 10% interstitial Mortality Decreasing With Better Detection Surgical and Medical Treatment Available Recurrence Rate ~ 10-15% RISK FACTORS Maternal age Number of sexual partners Cigarette smoking Previous Ectopic Pregnancy PID (Gonorrhea, Chlamydia) Tubal Surgery or pelvic surgery Infertility and infertility treatment ICUD IVF SITES Ampulla (50%) Isthmus (20%) Cornua (< 2%) Ovary (< 2%) Abdomen (< 2%) Cervix (< 2%) Simultaneous intrauterine and ectopic pregnancies (heterotopics) occur in 1/3000 to 1/30000 pregnancies SYMPTOMS Amenorrhea (typically 6-8 weeks) Abdominal Pain Vaginal Bleeding (small amount) Syncope Pelvic Mass Shoulder tip pain 15% of the cases present acutely with abdominal pain, amenorrhea and haemodynamic compromise In most cases the history will be more chronic Arias-stella reaction EVALUATION AND DIAGNOSIS History and Physical Exam Blood investigations (CBC, blood group) Serial Quantitative HCG Ultrasound Laparoscopy EVALUATION AND DIAGNOSIS Clinical: O/E: look for signs of intra-peritoneal hemorrhage Abdominal tenderness(95%) Peritonism Abdominal distension Pain on movement of the cervix (cervical excitation (50%) Adnexal mass (63%) Cervix ----closed SERIAL B-HCG HCG Levels Double Every 48 Hrs 66% Rise / 48 Hrs Consistent With Ectopic Single Determination Not Helpful Best If Done Within Same Laboratory At HCG of 1000 IU/L gestational sac of an intrauterine pregnancy should be detected by US ULTRASOUND May or May Not Be Helpful Discriminatory Zone: TV: 1500-2000 mIU/ml TA: 6500 mIU/ml +IUP: Generally Excludes Ectopic Free fluids in POD Adnexal mass TREATMENT Observation Laparoscopy Laparotomy Medical MTX Hyperosmolar Glucose PG OBSERVATION Many Tubal Pregnancies Abort Needs simple follow up Criteria for selection of patients Serial HCG levels and US MANAGEMENT OF ACUTE HEMORRHAGE - - Urgent hospital assessment Resuscitation Intravenous access and two large cannula Start IVF (colloid) Send for blood group, CBC and cross match Serum BHCG Transfer to theater Anti D should be given to all RH negative women LAPAROSCOPY Allows Diagnosis and Treatment Lower post op morbidity and quicker recovery Salpingotomy Salpingectomy (Total / Partial) Cornual Resection Minimally Invasive, Unlike Laparotomy Few Contraindications: Unstable Patient (Possibly) MINI-LAPAROTOMY Salpingectomy Salpingotomy Needed in acute intra-peritoneal haemorrhage-------for immediate ligation of the bleeding point MEDICAL TREATMENT Suitable patients are: Haemodynamically stable serum BHCG less than 10000IU/L no extrauterine fetal heart by US compliant patient METHOTREXATE Toxic to Trophoblast Cells Minimal Side Effects May Preserve Fertility in Cases of Cervical Pregnancy Requires Compliant Patient, Time Pain Not Uncommon BHCG May Rise Initially PERSISTENT TROPHOBLAST Most Often after Salpingostomy Laparoscopic Minilap Most Easily Treated With MTX OUTCOMES 15% Repeat Ectopic Rate 60-70% intra-uterine pregnancy after single ectopic SUMMARY Ectopic Pregnancy is a Common, Treatable Problem Sensitive Assays Allow Early Detection Surgical and Medical Options Exist Ruptured Ectopics should be Unusual with Compliant Patients and Appropriate Medical Care THANKS