August - British Heart Rhythm Society
advertisement

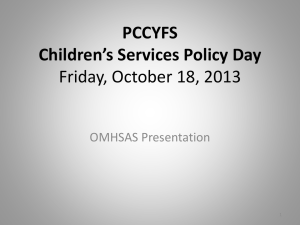
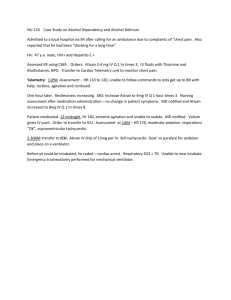
British Heart Rhythm Society Newsletter Summer 2014 Welcome to the BHRS Summer 2014 newsletter. There is a lot in this newsletter which I hope you will find interesting. Most importantly, there will be elections for doctor and physiologist representatives for Council. Please read this section and I would encourage you to consider standing if you want to help shape the future of BHRS. The release of NICE Technology Appraisal TA314 was a major improvement on the previous Appraisal and the changes are due, in no small part, to the input of Chris Plummer on behalf of BHRS. Read his commentary on what is covered and what is not! Francis Murgatroyd has worked hard on the new CRM databases which went live in April and he gives an update on the current status of the audit. He also covers meetings that have been held between BUPA and BHRS to discuss coding of procedures, amongst other things (of particular interest to consultant members). Sue Jones has been awarded an honorary Fellowship of the Royal College of Physicians and David Ward provides some background on Sue’s long-standing relationship with BHRS and also her work as a cardiac physiologist. There is still ongoing debate on the issue of conscious sedation in cardiology and our President, Steve Furniss, gives an update. We have 2 quizzes in this issue, a relatively straightforward one submitted by Barbara Bosch and a more difficult one from Sue Jones. If you wish to submit your own ideas or questions for the quiz, please send them to admin@bhrs.com. Please note the content of the quiz is the responsibility of the author and BHRS will not enter into correspondence on this matter. Finally, I hope you will be coming to this year’s Heart Rhythm Congress, (5 th – 8th October) at The ICC in Birmingham. Please make an effort to attend your Annual General Meeting which will be from 17:30 to 18:30 on Monday 6 th October in Hall 8B at the ICC. I look forward to seeing you there! Nick Linker President Elect ELECTIONS FOR COUNCIL This summer we will again be looking for some new blood for Council. We will need 2 physicians and 1 physiologist to replace current members who have reached the end of their tenure. This is your opportunity to get involved and bring your ideas to Council. Posts will be for three years initially, with the opportunity for a second term. Successful candidates will take up their seats at the AGM in October. In recent years we have not had a great deal of interest in these posts. We wish to make this a more vibrant organisation, responsive to your needs, with a louder voice and we need your help to do it, so please think about standing for Council! Please click here to download the nomination papers. Alistair Slade Secretary NEW NICE GUIDANCE ON ICDs AND CRT After a long gestation, NICE published new guidance on ICDs and CRT in June 2014 (http://www.nice.org.uk/Guidance/TA314). Combining the two previous appraisals (TA095 for ICDs and TA120 for CRT) is clinically appropriate, but the complexity of the process was clearly challenging for the committee. Click here for the full commentary. Chris Plummer BHRS representative for NICE TA314 NATIONAL CARDIAC RHYTHM MANAGEMENT AUDIT As you will be aware, the new national datasets came into place on 1st April 2014. If you haven’t seen it please read the letter that was sent out in July to all clinical leads and data managers. This addresses, amongst other things: Deadlines for data submission (in line with all other national cardiac audits, this is now quarterly) The imminent closure to submissions to the old dataset. Clarification of two critically important fields (intervention type, maximum system capability) The need for all operators and supervising consultants to be identified by GMC number (again, this is in line with other national audits) Please be aware (and make your colleagues aware) that the annual report for 2014-15 and the website will be reporting procedure numbers by hospital and by consultant. If the “intervention type” and the GMC number are not there, they will not appear on the reports and this may have effects on commissioning, revalidation, etc. The CRM audit page of the BHRS website will go live in August. As you will know, Morag (morag.cunningham@ucl.ac.uk) and I have been fielding requests for clarification (“how do I complete this field when …” “what should this procedure/ECG be called?” etc.) and we will update the “notes” column by each field, so this will be available for all. Please keep your enquiries coming, it is the best way to improve the data. The CRM audit page will also have links to previous years’ annual reports, and in future to hospital- and consultant- based activity data. For now, we will have a link allowing hospitals and operators (consultants and trainees) to view their recent quarterly statistics, allowing them to resubmit their data if it is incorrect. Francis Murgatroyd Audit Lead CONSULTATIONS WITH BUPA As consultant members know, BUPA recently circulated providers (cardiologists) with requests for information and feedback. One request that has given rise to concern was that providers give a statement of their scope of practice: BHRS has not addressed this issue specifically but would draw providers’ attention to the recent letters from Iain Simpson, President of BCS. BUPA also sought feedback from their providers on new proposals for clinical coding of procedure complexity. It was not clear how these proposals had been drawn up but we were disappointed not to have been consulted (nor were the other subspecialty groups such as BCIS). The period of consultation was short so we have not consulted all members (who have in any case been approached directly by BUPA, and many have given feedback). However, we have had a constructive meeting with the cardiac lead for BUPA, at which the shortcomings of both the existing complexity codes and the new proposals were discussed in some detail. As a result we have drafted new proposals for both EP and device procedures, which have been agreed by all Consultant members of BHRS (who in turn were asked to sound out colleagues informally). We think these will address some of the significant issues (e.g. ablation of AF, typical flutter versus complex atrial arrhythmias, permutations of device procedures, lead extraction, etc.). We are awaiting a response from BUPA which may be an invitation to further meeting/negotiation. Francis Murgatroyd Audit Lead HONOUR FOR SUE JONES Sue Jones, one of our most active and long-serving members, who has been running the pacemaker department at St George’s for almost a quarter of a century, was recently awarded honorary Fellowship of the Royal College of Physicians. During her time at St George’s, she has enthusiastically embraced the introduction and evaluation of numerous new devices, methods of remote monitoring, complex pacing therapy and also first-in-man implantation of some prototype devices. The first pacemaker in the United Kingdom was implanted at St George’s Hospital at Hyde Park Corner over 50 years ago and it was a British invention. I first had the pleasure of working with Sue at Brompton in 1980 as a newly appointed senior registrar when she was Senior Chief Cardiac technician - as the terminology was in those days. Sue departed for a position in the devices industry after a few months but later returned to the NHS and was subsequently appointed in 1990 to lead the rapidly expanding pacemaker clinic at St George’s. By 1995 she had established a satellite network staffed by physiologists mostly trained by her. As a Senior Cardiac Physiologist she has made innovative contributions to management, procurement, training and teaching - including physiologists, scientists, medical students, cardiology trainees and consultants. Sue lectures at several Colleges and Universities in London and Surrey and is co-author on many research papers about cardiac pacing and electrophysiology. She has been a Council member of both BPEG and Heart Rhythm UK and in 2008 received a Lifetime Achievement award for services to pacing and patient support. Sue is also an active member and contributor to the certification committee of BHRS and has been active in the development of the certification process since its introduction. Her national reputation was already established when in 1997 she founded the first forum for patients with implanted cardiac defibrillators. It is appropriately called BACKUP and is now affiliated to the charity Arrhythmia Alliance of which Sue is a Trust board member. This forum has become a model for other pacemaker clinics across the United Kingdom and abroad. Sue received a Special Achievement Award from St George’s Hospital in 2007. David E Ward FRCP BHRS member since 1985 SAFE SEDATION IN CARDIOLOGY Yes, the sedation story goes on! As you may know I sat for two years on the Academy of Royal Colleges Committee that recently produced a report on safe sedation. The report was driven by anaesthetists and focused particularly on issues that had arisen in dental and GI sedation. However, there are several important consequences for us. One principle agreed is that sedation should be competency based (rather than based on a job-title) and I have produced a document with the chair of that committee outlining some guidance for cardiology sedation. There has been very considerable opposition, as you might expect and unfortunately the document is still in draft form but there are a few key principles about sedation for arrhythmia procedures to whet your appetite: Competencies for sedation are to be defined Outcomes of sedation should be recorded and audited The “operator-sedationist” model is not appropriate (i.e. a dedicated person in charge of the sedation is essential) Nurse-administered propofol is appropriate for some cases but with restrictions: - Only via TCI pumps - Only with capnography monitoring - Only with ALS trained nurses - Only if patient has no features to indicate possible difficulty with airway maintenance Nurse competencies will have to be maintained on a regular basis Each Trust will need to set up a sedation committee into which there will be GI and cardiology input I realise that there are cost implications in new equipment and for some of your institutions these changes will be a step too far whilst others already deliver very effective sedation in a medical model and adoption of a nurse-led model is deemed irrelevant. However, I believe that for many this may open the door for a significant improvement in the quality of care we are able to deliver our patients and will also enable development of much more efficient services in many parts of the country. I hope soon to be able to bring you good news about the document being published. Steve Furniss President ECG QUIZ A 32 year old woman presented with a 4 year history of worsening palpitations. The palpitations usually occur shortly after exercise and also when she goes to bed. This ECG was obtained whilst she had her typical symptoms. Which of the following is the most likely diagnosis? A. B. C. D. E. Atrial fibrillation with ventricular pre-excitation Atrial tachycardia in a patient with Wolff Parkinson White syndrome Right ventricular outflow tract ventricular tachycardia Supraventricular tachycardia with left bundle branch block Ventricular tachycardia arising from the left posterior fascicle (Question provided by Barbara Bosch) View Answer QUIZ These tracings were taken from a St Jude Medical Victory DR pacemaker implanted in a 35 year old man for complete heart block in 2006. He had some wound problems and a revision in 2008 but was relatively trouble free. He reported occasional palpitations and at follow-up was seen to have occasional appropriate mode switching for very short runs of tachycardia. He was not anti-coagulated as his risk factors were low. He requested an early appointment with symptoms of palpitations and heart pounding over 4 days. The programmed parameters and diagnostics (Figure 1) are shown together with the presenting ECG and electrograms (Figure 2) plus an ECG and electrograms after programming (Figure 3). To see in a higher resolution, please click on the individual images. Figure 1 Figure 2 Figure 3 Which of the following is the most likely parameter to have been changed? A. B. C. D. E. AV delay PVAB PVARP Mode switch rate Upper rate limit (Question provided by Sue Jones) View Answer