Anemia_abstract_040814_MSS_XH
advertisement

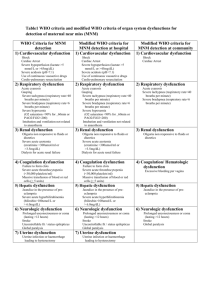
Anemia and end-organ dysfunction in critically ill medical and surgical ICU patients Author list Sarah Hemauer Adam J. Kingeter Xue Han Matthew S. Shotwell Pratik P. Pandharipande Liza M. Weavind Department of Anesthesiology and Biostatistics, Vanderbilt University Medical center, Nashville, TN Background: Anemia is associated with increased morbidity and mortality, however, transfusion of packed red blood cell (PRBC) is also an independent predictor of worse clinical outcomes. Recent data have supported the safety of restrictive transfusion strategies with a resultant decrease in PRBC use and acceptance of anemia, yet little is known about the impact of this anemia on the daily risk of individual organ dysfunctions in medical and surgical ICU patients. Methods: We performed a post-hoc analysis of prospectively collected data from the BRAINICU observational cohort study of medical and surgical ICU patients admitted with respiratory failure or shock. Baseline demographic data as well as detailed in-ICU and hospital data, including daily hemoglobin levels, were collected in the study up to hospital Day 30. Patients were evaluated daily for brain dysfunction (delirium) using the CAM-ICU, for renal dysfunction using the renal SOFA score (based on creatinine and urinary output) and for respiratory dysfunction using the respiratory SOFA score (based on the PaO2/FiO2 ratio) or need for mechanical ventilation. We also collected data on in-hospital mortality and calculated time to death. The adjusted associations between the current day hemoglobin level and organ dysfunction the following day were assessed using multinomial, ordinal (proportional odds), and binary logistic regression Cox proportional hazards regression with time-varying covariates was used to assess the adjusted association between current day hemoglobin and time to death. In each analysis, we adjusted for covariates including age, the APACHE II score, Charlson comorbidity index, Framingham stroke risk profile, ICU day, ICU type (medical vs. surgical), current sepsis, current organ dysfunction, and current lowest hemoglobin level... Statistical significance was indicated for p-values less than 0.05, or for 95% confidence intervals that fail to include the relevant null value. Results: We enrolled 821 patients with a median (interquartile, IQR) age of 61 (51, 71), APACHE II score of 21 (15, 26) and 30% septic on enrollment. Current lowest hemoglobin level was significantly associated with respiratory SOFA score the following day. For each increasing unit of the current lowest hemoglobin measurement, the odds of more severe respiratory SOFA score the following day were decreased by 30.6% (95% CI: 16.0, 62.7). This protective effect was significantly reduced in patients with greater current respiratory SOFA score (p-value: <0.001). There was no evidence of an association between current hemoglobin level and brain dysfunction, renal dysfunction, or the odds of mechanical ventilation the following day, or time to death. Conclusion: In this study population, lower hemoglobin levels were not associated with daily risk of development of brain or renal dysfunctions, or death. However, lower hemoglogin levels were associated with more severe respiratory dysfunction, as indicated by the respiratory SOFA criteria (lesser PaO2/FiO2 ratio and mechanical ventilation)