Morse Fall Risk Assessment Tool
advertisement

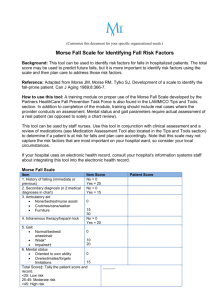
Morse Fall Risk Assessment Tool Fall Risk is based upon Fall Risk Factors and it is more than a Total Score. Determine Fall Risk Factors and Target Interventions to Reduce Risks. Complete on all patients at admission, at change of condition; transfer to a new unit, and after a fall. Please enter dates as follows: Feb. 12, 2012 (Mmm. DD, YYYY) Part A: Score Morse Fall Risk Assessment Tool NO 0 YES 25 Secondary Diagnosis NO 0 YES 25 Ambulatory Aid History of Falling None/bedrest/nurse assist 0 Crutches/cane/walker 15 Furniture 30 Gait Review Date: Review Date: Review Date: NO 0 YES 25 IV or IV access Mental Status Admission Date: Normal/bedrest/wheelchair 0 Weak 10 Impaired 20 Knows own limits 0 Overestimates or forgets limits 15 Total Initial To obtain the Morse Fall Score add the score from each category Morse Fall Score High Risk 45 and higher Moderate Risk 25-44 Low Risk 0-24 Feb. 2012 1of 2 Fall Prevention and Management Intervention Careplan YES NO Date: ___________ Initial ______ Fall Prevention/Intervention Careplan resolved YES NO Date: ___________ Initial ______ Fall Prevention/Intervention Careplan initiated Part B: Fall Prevention and Management Intervention Careplan (Nurse to date and initial any changes made following reassessment) Level 1 Interventions Level 2 Interventions Implement all of the following interventions (check to implement the appropriate interventions below) Identify Patient with a blue wristband Physio Therapy (PT) referral PT Recommendations Identify Patient with a blue Fall Prevention Sign ________________________________________________ Provide patient with non-skid socks ________________________________________________ ________________________________________________ Patient will have at least one side rail down (bottom left rail) Move Patient closer to nurses desk if at all possible Patient/Family will be provided with education on the FPMP. Have Patient/Family sign on data base that they have received education Occupational Therapy (OT) Referral OT Recommendations ________________________________________________ ________________________________________________ ________________________________________________ Mediation review Toileting routine Bed alarm Wheelchair with rear closing seat belt PRN Restraints Constant care/Family to stay with Patient Mat on floor Feb. 2012 2of 2