Introduction to anatomy and terminology
advertisement

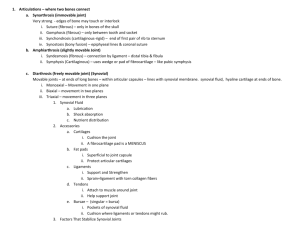
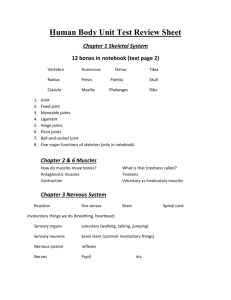
Dr. Kaan Yücel http://yeditepedentistryanatomy.wordpress.com Yeditepe Anatomy 24.November.2011 Thursday Introduction to Anatomy The word “anatomy” is derived from “anatomia, anatome” which has a Latin and Ancient Greek origin. The prefix “ana-“means “up", where “temnein, tome” means "to cut." As a result, anatomy means “cutting up, cutting through”. The term human anatomy comprises a consideration of the various structures which make up the human organism. Human anatomy deals with the structure of the human body at the gross, cellular, and subcellular levels. It also deals with the way in which development and growth alter structure and with relationships between structure and function. A knowledge of these topics is essential for anyone who wishes to become a clinical practitioner and this is especially so for those whose practise is likely to be of a surgical nature. It is impossible to understand the effects of diseases and their clinical manifestations without an understanding of healthy structure and function; nor it is possible to intervene effectively and safely with surgical procedures, in order to cure a diseases, without a good working knowledge of the anatomy of the relevant part of the body. Types of anatomy The three main approaches to studying anatomy are regional, systemic, and clinical (or applied), reflecting the body's organization and the priorities and purposes for studying it. In systematic anatomy, various structures may be separately considered—and the organs and tissues may be studied in relation to one another in topographical or regional anatomy. Regional Anatomy Regional anatomy (topographical anatomy) considers the organization of the human body as major parts or segments: a main body, consisting of the head, neck, and trunk (subdivided into thorax, abdomen, back, and pelvis/perineum), and paired upper limbs and lower limbs. All the major parts may be further subdivided into areas and regions. Regional anatomy is the method of studying the body's structure by focusing attention on a specific part (e.g., the head), area (the face), or region (the orbital or eye region); examining the arrangement and relationships of the various systemic structures (muscles, nerves, arteries, etc.) within it; and then usually continuing to study adjacent regions in an ordered sequence. Surface anatomy is an essential part of the study of regional anatomy. Surface anatomy provides knowledge of what lies under the skin and what structures are perceptible to touch (palpable) in the living body at rest and in action. In short, surface anatomy requires a thorough understanding of the anatomy of the structures beneath the surface.. Systematic Anatomy Systematic Anatomy.—The various systems of which the human body is composed are grouped under the following headings: Osteology—the bony system or skeleton. Syndesmology—the articulations or joints. Myology—the muscles. With the description of the muscles it is convenient to include that of the fasciæ which are so intimately connected with them. Angiology—the vascular system, comprising the heart, bloodvessels, lymphatic vessels, and lymph glands. Neurology—the nervous system. The organs of sense may be included in this system. Splanchnology—the visceral system. Topographically the viscera form two groups, viz., the thoracic viscera and the abdomino-pelvic viscera. The heart, a thoracic viscus, is best considered with the vascular system. The rest of the viscera may be grouped according to their functions: (a) the respiratory apparatus; (b) the digestive apparatus; and (c) the urogenital apparatus. Strictly speaking, the third subgroup should include only such components of the urogenital apparatus as are included within the abdomino-pelvic cavity, http://www.twitter/yeditepeanatomy 1 Dr. Kaan Yücel http://yeditepedentistryanatomy.wordpress.com Yeditepe Anatomy but it is convenient to study under this heading certain parts which lie in relation to the surface of the body, e. g., the testes and the external organs of generation. Clinical Anatomy Clinical (applied) anatomy emphasizes aspects of bodily structure and function important in the practice of medicine, dentistry, and the allied health sciences. It incorporates the regional and systemic approaches to studying anatomy and stresses clinical application. History of dentistry and anatomy in dentistry The development of anatomy as a science extends from the earliest examinations of sacrificial victims to the sophisticated analyses of the body performed by modern scientists. It has been characterized, over time, by a continually developing understanding of the functions of organs and structures in the body. The field of Human Anatomy has a prestigious history, and is considered to be the most prominent of the biological sciences of the 19th and early 20th centuries. Methods have also improved dramatically, advancing from examination of animals through dissection of cadavers to technologically complex techniques developed in the 20th century. It is believed that the oldest civilization that knew something of dentistry was Egypt. The earliest indication of such knowledge is found in the Edwin Smith Surgical Papyrus. It contains detailed directions for the treatment of wounds about the mouth, but no mention is made of restoring lost teeth resulting from these injuries. The hard tissues of the mouth were in general considered untreatable. In closing his discussion on this topic one ancient Egyptian surgeon advises: "One having a fracture of the mandible over which a wound has been inflicted and he has fever from it, it is an ailment not to be treated". The first known dentist was an Egyptian named Hesi-Re (3000 B.C.). He was the chief toothist to the Pharaohs. He was also a physician, indicating an association between medicine and dentistry. Most of the great surgeons had no knowledge of Anatomy but their teachings were not refuted untilVesalius, 1500 of Belgium, rebelled and became an anatomist at the University of Padua, Italy. He freed the mind of the medical profession and laid the foundation for true scientific research which is the basis of our present day medical practice. He accurately described the teeth and pulp chambers. Fallopius was another anatomist, a pupil of Vesalius. He is credited with the descriptions of the dental follicle, tri-geminal nerve, auditory nerve, LX nerve, the glosso pharyngeal, and hard and soft palate. He stated that teeth were not true bone. During the 1500s, advances in anatomy, microbiology, and other areas laid the foundations for specialized treatises on dentistry and for a theoretical—not just mechanical and empirical—approach to oral health. These advances included detailed anatomical descriptions of teeth and related structures. In 1771, John Hunter published "The natural history of human teeth" giving a scientific basis to dental anatomy. The book can be reviewed at the following link: http://books.google.com/books?id=_1BhAAAAIAAJ&printsec=frontcover&hl=tr&source=gbs_ge_summar y_r&cad=0#v=onepage&q&f=false The history of dental education is marked by both change and continuity. As dental science and technology have advanced, instruction in dental practice has become more sophisticated both in substance and in method. During the last century and a half, training through apprenticeship—and purely self-taught and self-proclaimed competency—have been replaced by a lengthy period of formal instruction. By the 21st century, the availability of interactive computer programs and changing public sentiment led to renewed debate on the use of cadavers in medical education. The Peninsula College of Medicine and Dentistry in the UK, founded in 2000, became the first modern medical school to carry out its anatomy education without dissection, though most medical schools continue to see experience with actual cadavers as preferable to entirely computer-based education. Suggested Readings http://www.scribd.com/doc/29704226/History-of-Dentistry http://www.drfaragdental.com/history.asp http://www.namibiadent.com/History/HistoryDentistry.html Anatomical Position All anatomical descriptions are expressed in relation to one consistent position, ensuring that descriptions are not ambiguous. One must visualize this position in the mind when describing patients (or cadavers), whether they are lying on their sides, supine (recumbent, lying on the back, face upward), or prone (lying on the abdomen, face downward). http://www.youtube.com/yeditepeanatomy 2 Dr. Kaan Yücel http://yeditepedentistryanatomy.wordpress.com Yeditepe Anatomy The anatomical position refers to the body position as if the person were standing upright with the: head, gaze (eyes), and toes directed anteriorly (forward), arms adjacent to the sides with the palms facing anteriorly, and lower limbs close together with the feet parallel. http://www.tpub.com/content/armymedical/MD0956/MD09560009.htm Anatomical Planes Anatomical descriptions are based on four imaginary planes (median, sagittal, frontal, and transverse) that intersect the body in the anatomical position: The median plane, the vertical plane passing longitudinally through the body, divides the body into right and left halves. The plane defines the midline of the head, neck, and trunk where it intersects the surface of the body. Midline is often erroneously used as a synonym for the median plane. Sagittal planes are vertical planes passing through the body parallel to the median plane. Frontal (coronal) planes are vertical planes passing through the body at right angles to the median plane, dividing the body into anterior (front) and posterior (back) parts. Transverse planes are horizontal planes passing through the body at right angles to the median and frontal planes, dividing the body into superior (upper) and inferior (lower) parts. Radiologists refer to transverse planes as transaxial, which is commonly shortened to axial planes. Any other plane of division is referred to as oblique. Oblique sections are slices of the body or any of its parts that are not cut along the previously listed anatomical planes. In practice, many radiographic images and anatomical sections do not lie precisely in sagittal, frontal, or transverse planes; often they are slightly oblique. Anatomical Variations Anatomy books describe (initially, at least) the structure of the body as it is usually observed in people—that is, the most common pattern. However, occasionally a particular structure demonstrates so much variation within the normal range that the most common pattern is found less than half the time! Terminology in Anatomy It is important for medical personnel to have a sound knowledge and understanding of the basic anatomic terms. With the aid of a medical dictionary, you will find that understanding anatomic terminology greatly assists you in the learning process. Various adjectives, arranged as pairs of opposites, describe the relationship of parts of the body or compare the position of two structures relative to each other. Anatomical directional terms are based on the body in the anatomical position. Four anatomical planes divide the body, and sections divide the planes into visually useful and descriptive parts. Anatomical terms are specific for comparisons made in the anatomical position, or with reference to the anatomical planes: Superior refers to a structure that is nearer the vertex, the topmost point of the cranium (Mediev. L., skull). http://www.twitter/yeditepeanatomy 3 Dr. Kaan Yücel http://yeditepedentistryanatomy.wordpress.com Yeditepe Anatomy Cranial relates to the cranium and is a useful directional term, meaning toward the head or cranium. Inferior refers to a structure that is situated nearer the sole of the foot. Caudal (L. cauda, tail) is a useful directional term that means toward the feet or tail region, represented in humans by the coccyx (tail bone), the small bone at the inferior (caudal) end of the vertebral column. Posterior (dorsal) denotes the back surface of the body or nearer to the back. Anterior (ventral) denotes the front surface of the body. Medial is used to indicate that a structure is nearer to the median plane of the body. For example, the 5th digit of the hand (little finger) is medial to the other digits. Conversely, lateral stipulates that a structure is farther away from the median plane. The 1st digit of the hand (thumb) is lateral to the other digits. Other terms of relationship and comparisons are independent of the anatomical position or the anatomical planes, relating primarily to the body's surface or its central core: Superficial, intermediate, and deep (Lat. Profundus, profunda) describe the position of structures relative to the surface of the body or the relationship of one structure to another underlying or overlying structure. External means outside of or farther from the center of an organ or cavity, while internal means inside or closer to the center, independent of direction. Proximal and distal are used when contrasting positions nearer to or farther from the attachment of a limb or the central aspect of a linear structure (origin in general), respectively. For example, the arm is proximal to the forearm and the hand is distal to the forearm. Invaginations and evaginations are inward and outward bulges in the wall of a cavity. Terms of Laterality Paired structures having right and left members (e.g., the kidneys) are bilateral, whereas those occurring on one side only (e.g., the spleen) are unilateral. Something occurring on the same side of the body as another structure is ipsilateral; the right thumb and right great (big) toe are ipsilateral, for example. Contralateral means occurring on the opposite side of the body relative to another structure; the right hand is contralateral to the left hand. Terms of Movement Various terms describe movements of the limbs and other parts of the body. Most movements are defined in relationship to the anatomical position, with movements occurring within, and around axes aligned with, specific anatomical planes. While most movements occur at joints where two or more bones or cartilages articulate with one another, several non-skeletal structures exhibit movement (e.g., tongue, lips, eyelids). Terms of movement may also be considered in pairs of oppositing movements: Flexion and extension movements generally occur in sagittal planes around a transverse axis. Flexion indicates bending or decreasing the angle between the bones or parts of the body. For most joints (e.g., elbow), flexion involves movement in an anterior direction, but it is occasionally posterior, as in the case of the knee joint. Lateral flexion is a movement of the trunk in the coronal plane. Extension indicates straightening or increasing the angle between the bones or parts of the body. Extension usually occurs in a posterior direction. The knee joint, rotated 180° to other joints, is exceptional in that flexion of the knee involves posterior movement and extension involves anterior movement. Abduction is to draw away from the median plane, while adduction is to move towards the median plane. Circumduction is a combination of abduction, adduction, flexion and extension, e.g., circumduction can take place in joints like wrist, shoulder. To protrude or protract is to move forwards. To retrude or retract is to move backwards. To pronate is a specialized term meaning to turn the hand so that the palm faces backwards from the anatomical position. To suppinate is the opposite of pronate. Medial rotation (internal rotation) brings the anterior surface of a limb closer to the median plane, whereas lateral rotation (external rotation) takes the anterior surface away from the median plane. Elevation raises or moves a part superiorly, as in elevating the shoulders when shrugging, the upper eyelid when opening the eye, or the tongue when pushing it up against the palate (roof of mouth). http://www.youtube.com/yeditepeanatomy 4 Dr. Kaan Yücel http://yeditepedentistryanatomy.wordpress.com Yeditepe Anatomy Depression lowers or moves a part inferiorly, as in depressing the shoulders when standing at ease, the upper eyelid when closing the eye, or pulling the tongue away from the palate. http://learn-anatomy.blogspot.com/2009/06/terms-of-movement.html Positions of the body The supine position of the body is lying on the back. The prone position is lying face downward. OSTEOLOGY (BONES) Osteology (Gk, osteon, bone, logos, science) is the branch of medicine concerned with the development and diseases of bone tissue. The human skeleton is composed of 206 bones in adults. The skeletal system may be divided into two functional parts: The axial skeleton consists of the bones of the head (cranium or skull), neck (hyoid bone and cervical vertebrae), and trunk (ribs, sternum, vertebrae, and sacrum). The appendicular skeleton consists of the bones of the limbs, including those forming the pectoral (shoulder) and pelvic girdles. Bone is one of the hardest structures of the animal body, because of the calcification of its extracellular matrix. Living bones have some elasticity (results from the organic matter) and great rigidity (results from their lamellous structures and tubes of inorganic calcium phosphate). Its color, in a fresh state, is pinkish-white externally, and deep red within. Cartilage and Bones The skeleton is composed of cartilages and bones. Cartilage is a resilient, semirigid form of connective tissue that forms parts of the skeleton where more flexibility is required—for example, where the costal cartilages attach the ribs to the sternum. Also, the articulating surfaces (bearing surfaces) of bones participating in a synovial joint are capped with articular cartilage that provides smooth, low-friction, gliding surfaces for free movement. Blood vessels do not enter cartilage (i.e., it is avascular); consequently, its cells obtain oxygen and nutrients by diffusion. The proportion of bone and cartilage in the skeleton changes as the body grows; the younger a person is, the more cartilage he or she has. The bones of a newborn are soft and flexible because they are mostly composed of cartilage. Bones of the adult skeleton provide: support for the body and its vital cavities; it is the chief supporting tissue of the body. protection for vital structures (e.g., the heart). the mechanical basis for movement (leverage). storage for salts (e.g., calcium). a continuous supply of new blood cells (produced by the marrow in the medullary cavity of many bones). Bone has a protective function; the skull and vertebral column, for example, protect the brain and spinal cord from injury; the sternum and ribs protect the thoracic and upper abdominal viscera. It serves as a lever, as seen in the long bones of the limbs, and as an important storage area for calcium salts. It houses and protects within its cavities the delicate blood-forming bone marrow. A fibrous connective tissue covering which is called periosteum surrounds each skeletal element like a sleeve, except where articular cartilage occurs; whereas that around cartilage is perichondrium. The periosteum and perichondrium nourish the external aspects of the skeletal tissue. They are capable of laying http://www.twitter/yeditepeanatomy 5 Dr. Kaan Yücel http://yeditepedentistryanatomy.wordpress.com Yeditepe Anatomy down more cartilage or bone (particularly during fracture healing) and provide the interface for attachment of tendons and ligaments. Bones are classified according to their shape (gross anatomy): 1) Long bones are tubular (e.g., the humerus in the arm). 2) Short bones are cuboidal and are found only in the tarsus (ankle) and carpus (wrist). 3) Flat bones usually serve protective functions (e.g., the flat bones of the cranium protect the brain). 4) Irregular bones have various shapes other than long, short, or flat (e.g., bones of the face). 5) Sesamoid bones (e.g., the patella or knee cap) develop in certain tendons and are found where tendons cross the ends of long bones in the limbs; they protect the tendons from excessive wear and often change the angle of the tendons as they pass to their attachments. There are two types of bones according to histological features: compact bone and spongy (trabecular) bone. They are distinguished by the relative amount of solid matter and by the number and size of the spaces they contain All bones have a superficial thin layer of compact bone around a central mass of spongy bone, except where the latter is replaced by a medullary (marrow) cavity. Spongy bone is found at the expanded heads of long bones and fills most irregular bones. Compact bone forms the outer shell of all bones and also the shafts in long bones. The architecture and proportion of compact and spongy bone vary according to function. Compact bone provides strength for weight bearing. In addition, long bones have elevations (e.g., ridges, crests, and tubercles) that serve as buttresses (supports) where large muscles attach. Bone Markings and Formations Bone markings appear wherever tendons, ligaments, and fascias are attached or where arteries lie adjacent to or enter bones. Other formations occur in relation to the passage of a tendon (often to direct the tendon or improve its leverage) or to control the type of movement occurring at a joint. Surfaces of the bones are not smooth. Bones display elevations, depressions and holes. The surface features on the bones are given names to distinguish and define them. Some of the various markings and features of bones are: Linear elevation line, crest Round elevation tubercule (small eminence), protuberance (swelling) Sharp elevation spine, process Rounded articular area head, condyle Facets area with a smooth surface where a bone articulates with another bone Depressions fossae (small depression), groove (sulcus, long narrow depressions) Foramen hole Canal a foramen having length Orifice opening Meatus a canal entering a structure Vasculature and Innervation of Bones Bones are richly supplied with blood vessels. Veins accompany arteries. Nerves accompany blood vessels supplying bones. GENERAL CONSIDERATIONS ON JOINTS Syndesmology (Greek expression band, bond –logy) is the medical discipline where joints and ligaments of the body are studied. Joints (articulations) are unions or junctions between two or more bones http://www.youtube.com/yeditepeanatomy 6 Dr. Kaan Yücel http://yeditepedentistryanatomy.wordpress.com Yeditepe Anatomy or rigid parts of the skeleton. Joints exhibit a variety of forms and functions. It is the fact that, whether or not movement occurs between them, it is still called a joint. Some joints have no movement, others allow only slight movement, and some are freely movable, such as the glenohumeral (shoulder) joint Classification of Joints Joints are classified according to the tissues that lie between the bones: fibrous joints, cartilaginous joints, and synovial joints. Fibrous joints: The bones are united by fibrous tissue. The amount of movement occurring at a fibrous joint depends in most cases on the length of the fibers uniting the articulating bones. The sutures of the cranium are examples of fibrous joints. These bones are close together, either interlocking along a wavy line or overlapping. A syndesmosis type of fibrous joint unites the bones with a sheet of fibrous tissue, either a ligament or a fibrous membrane. Consequently, this type of joint is partially movable. The interosseous membrane in the forearm is a sheet of fibrous tissue that joins the radius and ulna in a syndesmosis. A dentoalveolar syndesmosis (gomphosis or socket) is a fibrous joint in which a peglike process fits into a socket articulation between the root of the tooth and the alveolar process of the jaw. Mobility of this joint (a loose tooth) indicates a pathological state affecting the supporting tissues of the tooth. Gomphosis is a joint that binds the teeth to bony sockets (dental alveoli) in the maxillary bone and mandible. The fibrous connection between a tooth and its socket is a periodontal ligament. Specifically, the connection is made between the maxillary or mandible to the cementum of the tooth. The gomphosis is the only joint-type in which a bone does not join another bone, as teeth are not technically bone. In modern, more anatomical, joint classification, the gomphosis is simply considered a fibrous joint because the tissue linking the structures is ligamentous. Small quantity of fibrous tissue holds the bones together. No movement is possible at such peg-and-socket joints. Gomphosis- Etymology: Gk, gomphos, gomphoein; bolt Sydesmosis- Etymology: It comes from the Greek σύν, syn (meaning "with") and δεσμός, desmos (meaning "a band"). Cartilaginous joints: The bones are united by hyaline cartilage or fibrocartilage. In primary cartilaginous joints, or synchondroses, the bones are united by hyaline cartilage, which permits slight bending during early life. Primary cartilaginous joints are usually temporary unions, such as those present during the development of a long bone, where the bony epiphysis and the shaft are joined by an epiphysial plate. Primary cartilaginous joints permit growth in the length of a bone. When full growth is achieved, the epiphysial plate converts to bone and the epiphyses fuse with the diaphysis. Secondary cartilaginous joints, or symphyses, are strong, slightly movable joints united by fibrocartilage. The fibrocartilaginous intervertebral discs between the vertebrae consist of binding connective tissue that joins the vertebrae together. Synovial joints: The bones are united by a joint (articular) capsule (composed of an outer fibrous layer lined by a serous synovial membrane) spanning and enclosing an articular cavity. Synovial joints are the most common type of joints and provide free movement between the bones they join; they are joints of locomotion, typical of nearly all limb joints. This type of joints has three common features: 1) Joint cavity: The joint cavity of a synovial joint, like the knee, is a potential space that contains a small amount of lubricating synovial fluid, secreted by the synovial membrane. 2) Articular cartilage: The articular surfaces are covered by hyaline cartilage. 3) Articular capsule: This structure surrounds the joint and formed of two layers. Inside the capsule, articular cartilage covers the articulating surfaces of the bones; all other internal surfaces are covered by synovial membrane. a) Fibrous capsule: It protects and gives firmness to the joint stability, continues with the periosteum b) Synovial membrane: It lines the inner surface of the fibrous membrane but does not cover the articular cartilage. The synovial membrane secretes a fluid known as synovial fluid. This fluid helps to minimize the friction by articular sufaces. Some synovial joints have other distinguishing features, such as a fibrocartilaginous articular disc or meniscus, which are present when the articulating surfaces of the bones are incongruous. http://www.twitter/yeditepeanatomy 7 Dr. Kaan Yücel http://yeditepedentistryanatomy.wordpress.com Yeditepe Anatomy Ligaments: A ligament is a cord or band of connective tissue uniting two structures. Articular capsules are usually strengthened by articular ligaments. These are from dense connective tissue and they connect the articulating bones to each other. Articular ligaments limit the undesired and/or excessive movements of the joints. Articular ligaments are classified as intrinsic and extrinsic ligaments. Intrinsic ligaments are the thickening of a portion of the articular capsule. Articular disc: Help to hold the bones together. The articular disc separates synovial cavities. This separation of the cavity space allows for separate movements to occur in each space. For example, the temporomandibular joint has an articular disc which divides the joint into two separate cavities. Labrum: A fibrocartilaginous ring which deepens the articular surface for one of the bones. Fatt Pads: A pad of fat lying within a joint, covered with synovial membrane and thought to assist in the spreading of synovial lubricant, e.g. infrapatellar fat pad of stifle joint. Bursae: Bursae are flattened sacs that contain synovial fluid to reduce friction. Its walls are separated by a film of viscous fluid. Bursae are found wherever tendons rub against bones, ligaments, or other tendons. They are commonly found close to joints where the skin rubs against underlying bony structures, for example, the prepatellar bursa. Occasionally, the cavity of a bursa communicates with the cavity of a synovial joint. For example, the suprapatellar bursa communicates with the knee joint and the subscapularis bursa communicates with the shoulder joint. Tendon Sheath: A tendon sheath is a layer of the synovial membrane around a tendon. It permits the tendon to move. Types of synovial joints The six major types of synovial joints are classified according to the shape of the articulating surfaces and/or the type of movement they permit: 1. Plane joints (gliding joints) permit gliding or sliding movements in the plane of the articular surfaces. The articular surfaces of the plane joints are almost flat. 2. Hinge joints, permit flexion and extension only, around the transverse axis. Bones are joined with strong collateral ligaments. 3. Saddle joints permit abduction and adduction as well as flexion and extension, movements occurring around two axes at right angles to each other. 4. Condyloid joints permit flexion and extension as well as abduction and adduction. 5. Ball and socket joints allow movement in multiple axes and planes: flexion and extension, abduction and adduction, medial and lateral rotation, and circumduction. 6. Pivot joints permit rotation around a central axis. Stability of Joints The stability of a joint depends on four main factors: The negative pressure within the joint cavity, the shape, size, and arrangement of the articular surfaces; the ligaments; and the tone of the muscles around the joint. Joint vasculature and innvervation Joints receive blood from articular arteries that arise from the vessels around the joint. The arteries often anastomose (communicate) to form networks (periarticular arterial anastomoses) to ensure a blood supply to and across the joint in the various positions assumed by the joint. Articular veins are communicating veins that accompany arteries (L. venae comitantes) and, like the arteries, are located in the joint capsule, mostly in the synovial membrane. Joints have a rich nerve supply provided by articular nerves with sensory nerve endings in the joint capsule. The capsule and ligaments receive an abundant sensory nerve supply. A sensory nerve supplying a joint also supplies the muscles moving the joint and the skin overlying the insertions of these muscles, a fact that has been codified as Hilton's law. http://www.youtube.com/yeditepeanatomy 8