Methods
advertisement

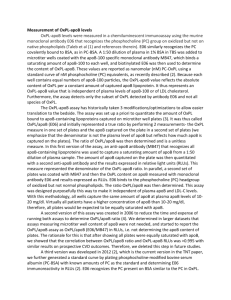
Online Supplementary Materials Oxidized Phospholipids, Lipoprotein(a) and Progression Of Calcific Aortic Valve Stenosis AUTHORS: Romain Capoulade, PhD, Kwan L. Chan, MD, FRCPC, Calvin Yeang, MD, PhD, Patrick Mathieu, MD, FRCSC, Yohan Bossé, PhD, Jean G. Dumesnil, MD, FRCPC, FACC, James W. Tam, MD, FRCPC, Koon K. Teo, MBBCh, PhD, FACC, Ablajan Mahmut, MD, MSc, Xiaohong Yang BSc, Joseph L. Witztum, MD, Benoit J. Arsenault PhD, Jean-Pierre Després, PhD, FAHA, Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE, Sotirios Tsimikas, MD, FACC 1 Online Supplementary Methods Clinical data Clinical data included age, gender, height, weight, waist circumference, body surface area (BSA), body mass index (BMI), systolic and diastolic blood pressures, hypertension (patients receiving antihypertensive medications or having known but untreated hypertension [blood pressure ≥ 140/90 mm Hg]), history of smoking and randomization status (i.e. statin vs placebo). The clinical identification of patients with the features of the metabolic syndrome (MetS) was based on the modified criteria proposed by the National Cholesterol Education Program – Adult Treatment Panel III (1). Doppler echocardiographic data The sonographers at each site received training in the acquisition and interpretation of the echocardiograms before the beginning of the study. Randomly selected studies that contributed 10% of the total number of echocardiograms were reviewed to ensure that the studies and measurements were performed in accordance with the protocol. Aortic valve morphology and function: The aortic valve (AV) phenotype (i.e. bicuspid vs. tricuspid) was recorded. The Doppler echocardiographic indices of AS severity included peak aortic jet velocity (Vpeak), peak and mean transvalvular pressure gradients obtained with the use of the modified Bernoulli equation, and the aortic valve area (AVA) calculated by the standard continuity equation. The AVA could not be determined in 16% (n=35) of the patients due to subvalvular flow acceleration or 2 inadequate measure of LV outflow tract diameter. The degree of AV calcification was scored according to the criteria proposed by Rosenhek et al (2). Left ventricular geometry and function: LV ejection fraction (LVEF) was measured with the use of biplane Simpson method. The relative wall thickness ratio was calculated by dividing the sum of the LV posterior wall and inter-ventricular septal thicknesses by the LV internal dimension (3). Left ventricular mass was calculated with the corrected formula of the American Society of Echocardiography and was indexed to a 2.7 power of height (3, 4). As a measure of global LV hemodynamic load, we calculated the valvulo-arterial impedance (5): Zva=(SBP+ΔPmean)/SVi where SBP is the systolic blood pressure, ∆Pmean the mean transvalvular gradient, and SVi is the stroke volume indexed to a 2.04 power of height (4). Measurement of OxPL-apoB, OxPL-apo(a) and Lp(a) levels OxPL-apoB levels were measured with a chemiluminescent immunoassay using the murine monoclonal antibody E06 that recognizes the phosphocholine (PC) group on oxidized but not on native phospholipids (6-10). E06 similarly recognizes the PC covalently bound to bovine serum albumin (BSA) in PC-BSA. A 1:50 dilution of plasma in 1% BSA in TBS was added to microtiter wells coated with the apoB-100 specific monoclonal antibody MB47, which binds a saturating amount of apoB-100 to each well, and biotinylated E06 was then added to determine the content of OxPL-apoB. These values are reported as nanomolar (nM) PC-OxPL using a standard curve of nM PC equivalents, as recently described (11). Because each well contains equal numbers of apoB-100 particles, the OxPL-apoB value reflects the absolute content of OxPL per a 3 constant amount of captured apoB lipoprotein. It thus represents an OxPL-apoB value that is independent of plasma levels of apoB-100 or LDL cholesterol. Furthermore, the assay detects only the subset of OxPL detected by antibody E06 and not all species of OxPL. In prior studies, this variable was expressed as OxPL/apoB, reflecting the fact that this measure quantitates the number of OxPL moles per unit mass of apolipoprotein B-100 present on microtiter well plates (and not the level in the circulation). The nomenclature is now changed to OxPL-apoB to minimize confusion that this measure represents a ratio of OxPL divided by plasma levels of apoB. Within-person 5-year reproducibility of frozen samples has been shown to be high (r=0.78) (12) and pilot-tests showed that OxPL-apoB levels are stable over 24 hours on ice (intraclass correlation coefficient 0.96) (11) as well as frozen samples stored under long term conditions (1315). OxPL-apo(a) levels were measured in an analogous manner to OxPL-apoB, except that the capture antibody, LPA4 (16), which detects apolipoprotein(a) was used to capture apo(a). The values are also reported in nM. Because these assays gave similar results to OxPL-apoB, the OxPL-apo(a) data are only shown in the Supplement. Please note that the absolute amounts of apoB-100 and apo(a) captured on the wells in the respective assays are different and therefore one can not directly compare the absolute OxPL-apoB and OxPL-apo(a) values. Lp(a) levels were measured by a validated chemiluminescent ELISA as previously described (6). 4 Online Supplementary Results Progression rate of aortic valve area The results of the analysis of the progression rate of AVA (i.e. annualized AVA progression rate) were strongly similar to those reported for the progression rate of Vpeak. Patients in the top tertile of Lp(a) had significantly faster progression of AVA compared to those in the middle and bottom tertiles (-0.08±0.11 vs. -0.04±0.12 cm²/yr, p=0.03). Patients in the top tertile of OxPL-apoB also displayed significantly faster stenosis progression than those in the middle and bottom tertiles (-0.09±0.10 vs. 0.04±0.12 cm²/yr, p=0.01). After multivariable analysis, using similar models as for Vpeak, top tertiles of Lp(a) or OxPL-apoB remained independently associated with AVA progression rate (all p<0.05). In patients ≤57 years, the results were also highly consistent with those reported with Vpeak: patients in the top tertile of Lp(a) or OxPL-apoB had faster stenosis progression (annualized AVA: -0.10±0.13 vs. -0.02±0.12 cm²/yr, p=0.003; -0.10±0.13 vs. -0.02±0.12 cm²/yr, p=0.002; respectively), and these relationships remained significant after multivariable adjustment (all p<0.05). Relationship of OxPL-apo(a) with AS progression rate and clinical outcomes The relationship between OxPL-apo(a) and AS progression rate or clinical outcomes were similar to those obtained with OxPL-apoB. In the overall group, median OxPL-apo(a) levels were 15.7 [4.5-51.7] nM and OxPL-apo(a) levels were strongly correlated to OxPL-apoB levels (r=0.86; p<0.001). Patients in the top tertile of OxPL- 5 apo(a) (>33.5 nM) had significantly faster stenosis progression compared to those in the middle and bottom tertiles (+0.26±0.26 vs. +0.17±0.21 m/s/yr, p=0.005). After multivariable analysis, using similar models as for OxPL-apoB (Multivariable Model #1, Table 2), OxPL-apo(a) remained independent predictors of faster progression rate of Vpeak (top tertile of OxPL-apo(a): βeta coeff.=0.22±0.04, p=0.02). Patients in the top tertile of OxPL-apo(a) had a higher risk of being rapid progressors in univariable (OR=2.1; 95% CI 1.2-3.8; p=0.009) and multivariable (OR=2.8; 95% CI 1.4-5.4; p=0.002) analysis. There was a significant interaction between patient’s age and OxPL-apo(a) (p=0.05) for AS progression. Among patients with median age ≤57 years, AS progression was 2-fold faster in those in the upper tertile of OxPL-apo(a) (>33.5 nM) compared to middle and bottom tertiles (+0.26±0.32 vs. +0.13±0.17 m/s/yr, p=0.005). After multivariable adjustment, using similar models as for OxPL-apoB, OxPL-apo(a) remained a powerful and independent predictor of faster AS progression rate in patients ≤57 years (all p≤0.01). In the subset of patients ≤57 years, those in the top tertile of OxPL-apo(a) had a higher risk of being rapid progressors in univariable (OR=4.0; 95% CI 1.7-9.5; p=0.001) and multivariable (OR=5.6; 95% CI 1.8-16.8; p=0.002) analysis. After adjustment for age, male gender and baseline AS severity, patients in the top tertile of OxPL-apo(a) had a significantly higher risk of clinical events, in the overall group (HR: 1.8, 95% CI 1.0-3.3, p=0.049) and in the subset of patients ≤57 years (HR: 4.2, 95% CI 1.3-13.4, p=0.01). 6 Online Supplementary Figure ONLINE FIGURE S1: Impact of Aortic Valve Phenotype and Randomization Status on AS Progression Rate according to Plasma Levels of Lp(a) and OxPL-apoB. Caption: Comparison of annualized progression rate of peak aortic jet velocity after dichotomization by aortic valve phenotype (i.e. bicuspid vs. tricuspid; Panels A and B) or randomization status (i.e. statin vs. placebo; Panels C and D) in patients in the middle and bottom tertiles vs. top tertile of Lp(a) (i.e. Lp(a) ≤ vs. >58.5 mg/dL; Panels A and C) and OxPL-apoB (i.e. OxPL-apoB ≤ vs. >5.50 nM; Panels B and D). ApoB: apolipoprotein B; Lp(a): lipoprotein(a); OxPL: oxidized phospholipids; Vpeak: peak aortic jet velocity. ¶: p<0.05 compared to “Lp(a)≤50-Placebo” group; #: p<0.05 compared to “Tertiles 1 & 2 of OxPL-apoB-Placebo” group. Error bars represent the SEM. 7 Online Supplementary References 1. Expert panel. Executive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adults treatment panel III). JAMA 2001; 285:248692. 2. Rosenhek R, Binder T, Porenta G, et al. Predictors of outcome in severe, asymptomatic aortic stenosis. N Engl J Med 2000; 343:611-7. 3. Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the american society of echocardiography and the European association of cardiovascular imaging. J Am Soc Echocardiogr 2015; 28:1-39. 4. Pagé A, Dumesnil JG, Clavel MA, et al. Metabolic syndrome is associated with more pronounced impairment of LV geometry and function in patients with calcific aortic stenosis: A substudy of the ASTRONOMER trial. (Aortic Stenosis Progression Observation Measuring Effects of Rosuvastatin). J Am Coll Cardiol 2010; 55:1867-74. 5. Hachicha Z, Dumesnil JG, Pibarot P. Usefulness of the valvuloarterial impedance to predict adverse outcome in asymptomatic aortic stenosis. J Am Coll Cardiol 2009; 54:1003-11. 6. Taleb A, Witztum JL, Tsimikas S. Oxidized phospholipids on apoB-100-containing lipoproteins: a biomarker predicting cardiovascular disease and cardiovascular events. Biomark Med 2011; 5:673-94. 7. Leibundgut G, Arai K, Orsoni A, et al. Oxidized phospholipids are present on plasminogen, affect fibrinolysis, and increase following acute myocardial infarction. J Am Coll Cardiol 2012; 59:1426-37. 8. Arai K, Orsoni A, Mallat Z, et al. Acute impact of apheresis on oxidized phospholipids in patients with familial hypercholesterolemia. J Lipid Res 2012; 53:1670-8. 8 9. Tsimikas S, Willeit P, Willeit J, et al. Oxidation-specific biomarkers, prospective 15year cardiovascular and stroke outcomes, and net reclassification of cardiovascular events. J Am Coll Cardiol 2012; 60:2218-29. 10. Tsimikas S, Duff GW, Berger PB, et al. Pro-inflammatory interleukin-1 genotypes potentiate the risk of coronary artery disease and cardiovascular events mediated by oxidized phospholipids and lipoprotein(a). J Am Coll Cardiol 2014; 63:1724-34. 11. Bertoia ML, Pai JK, Lee JH, et al. Oxidation-specific biomarkers and risk of peripheral artery disease. J Am Coll Cardiol 2013; 61:2169-79. 12. Tsimikas S, Kiechl S, Willeit J, et al. Oxidized phospholipids predict the presence and progression of carotid and femoral atherosclerosis and symptomatic cardiovascular disease: five-year prospective results from the Bruneck study. J Am Coll Cardiol 2006; 47:2219-28. 13. Rodenburg J, Vissers MN, Wiegman A, et al. Oxidized low-density lipoprotein in children with familial hypercholesterolemia and unaffected siblings: effect of pravastatin. J Am Coll Cardiol 2006; 47:1803-10. 14. Kiechl S, Willeit J, Mayr M, et al. Oxidized phospholipids, lipoprotein(a), lipoproteinassociated phospholipase A2 activity, and 10-year cardiovascular outcomes: prospective results from the Bruneck study. Arterioscler Thromb Vasc Biol 2007; 27:1788-95. 15. Tsimikas S, Mallat Z, Talmud PJ, et al. Oxidation-specific biomarkers, lipoprotein(a), and risk of fatal and nonfatal coronary events. J Am Coll Cardiol 2010; 56:946-55. 16. Tsimikas S, Lau HK, Han KR, et al. Percutaneous coronary intervention results in acute increases in oxidized phospholipids and lipoprotein(a): short-term and longterm immunologic responses to oxidized low-density lipoprotein. Circulation 2004; 109:3164-70. 9 Investigators and Sites of the ASTRONOMER trial Kwan Leung Chan, Ian Burwash, University of Ottawa Heart Institute (Ottawa, ON) Susan Fagan, Bruce Sussex, HSC-General Hospital (St. John’s, NFLD) Chris Koilpillai, Bruce Josephson, QEII HSC (Halifax, NS) Jean G. Dumesnil, Philippe Pibarot, Quebec Heart Institute (Laval, QC) George Honos, Jewish General Hospital (Montreal, QC) Jean-Claude Tardif, Montreal Heart Institute (Montreal, QC) Michele Turek, The Ottawa Hospital – General Campus (Ottawa, ON) Trevor Robinson, Chi-Ming Chow, St. Michael’s Hospital (Toronto, ON) Sam Siu, Eric Yu; Toronto General Hospital (Toronto, ON) Cam Joyner, Chris Morgan, Sunnybrook HSC (Toronto, ON) Charles Tomlinson, Koon Teo, Hamilton HSC (Hamilton, ON) James Tam, David Mymin, Nasir Shaikh, Davinder Jassal, HSC Winnipeg (Winnipeg) Bibiana Cujec, University of Alberta Hospital (Edmonton, AB) Peter Giannoccaro, Brian Connelly, Peter Lougheed Centre (Calgary, AB) Kenneth O’Reilly, William Hui, Ted Fenske, Alan Jones, Randy Williams (Royal Alexander Hospital (Edmonton, AB) John Jue, Ken Gin, Pui-Kee Lee, Vancouver General Hospital (Vancouver, BC) Randall Sochowski, Dennis Morgan, Mangeet Mann, Ken Yvorchuk, Victoria Heart Institute (Victoria, BC) Stephen Pearce, S. Cheung, Raymond Dong, J.M. Kornder, Dante Manyari, Salima Shariff, Surrey Memorial Hospital (Surrey, BC) Stuart Smith, Clause Rinne, Westheights Cardiology Clinic (Kitchener, ON) Thao Huynh, Montreal General Hospital (Montreal, QC) Milan Gupta, David Borts, Anil Gupta, Nickie Bonafede, Brampton Research Associates (Brampton, ON) Shekhar Pandey, Cambridge Cardiac Care Centre (Cambridge, ON) 10