Health History and Current Complaint Questionnaire
advertisement

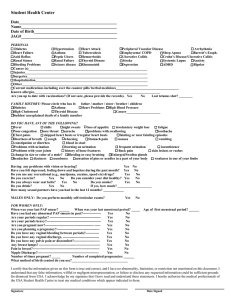
Name: _______________________________ Birthdate: ____________ Date: ____________ Reason for Visit: _______________________________________________________________ PLEASE READ ALL QUESTIONS AND ANSWER TO BEST OF YOUR KNOWLEDGE!!! Allergies: Medications Environmental Food None None Latex None Medications/Supplements (Regular or Occasional Use) : Please indicate name and dose None Medical/Surgical History: Current Past Condition/Disease Headaches, migraines, auras Eye problems, hearing loss Seizures/neurologic problems Strokes Depression, anxiety, mental disorders Thyroid disease Heart disease/heart attacks High blood pressure Mitral valve prolapse/ heart infection Blood clots in legs or lungs Excessive bleeding or bruising Anemia Blood transfusions Current Past Conditions/Disease High cholesterol, lipids Asthma, lung disease, tuberculosis Hepatitis, liver, gallbladder disease Diabetes Ulcers, heartburn, stomach problems Bladder or kidney infections Kidney Stones Muscle, bone, joint problems Breast problems, lumps, cancer Gynecologic problems Abnormal pap smears Surgeries, Accidents, Hospitalizations Other Screening History: Last Pap: _________(date)-normal or ______________________ High Risk HPV testing? ______________ Last Mammogram: __________ (date)-normal or ______________________________ Prior Cholesterol/Lipid Screening: _________ (date)-normal or _____________________________ Last Bone Density Scan: _________ (date)-normal or ______________________ Last Colonoscopy/Sigmoidoscopy: _________ (date)-normal or ___________________________ Gynecologic History: Menstrual: LMP (1st day) __________ Frequency (between 1st days) - ____ days Duration - ____days Regular Irregular Flow - light moderate heavy varies Bleeding between periods? No Yes Age period started - ___ years Pregnancy: Total Number Pregnancies - _____ Births - _____ Preterm - _____ Miscarriage - _____ Abortion - _____ Ectopic - _____ Vaginal - _____ C-Section - _____ Living Children-_____ Sexual: Orientation – Opposite sex Same sex Both Transgender – No Yes Current Partner(s) - No Yes Time with Partner(s) - ___ weeks months years Contraception: Current _____________________ Desired _______________________ None Infections (Circle): Gonorrhea Chlamydia Herpes (self/partner) Venereal Warts Hepatitis Syphilis HIV Trich BV Yeast Pelvic Inflammatory Disease MRSA (past 1 year) Trauma History Have you ever been sexually abused, raped or molested? No Yes Have you ever been in a psychologically or physically abusive relationship? No Yes Do you feel safe in your current relationship? Yes No Not currently in a relationship Family History Mother Father Sister Brother MatGM MatGF Maternal Aunts/Uncles PatGM PatGF Paternal Aunts/Uncles Child Hypertension Blood Clot/Stroke Heart attack High cholesterol Diabetes Breast cancer Ovarian cancer Colon cancer Osteoporosis Other Social/Lifestyle History: Marital Status: Single Married Separated Divorce Widowed Domestic Partner Tobacco History: Smoker - Never Former Quit _______ (date) Current ___Cigs/day x ___yrs Chews Alcohol: Never In past or ___drinks per day week month year Recreational Drugs: Never In past Current Substances: Exercise: No or ____ times per week for ____ minutes Light Moderate Heavy Current Symptoms: ROS General Skin Please circle all CURRENT complaints appetite loss chills fatigue weight gain/obesity weight loss nail changes dryness hair growth feels poorly fever other _____________ hair loss itching lesions rash other ____________ HEENT vision changes corrective lenses sore throat other ____________ Neck Respiratory Breast Cardiovascular Gastrointestinal pain stiffness swollen glands other____________ cough difficulties breathing snoring sputum wheezing other ______________ mass pain swelling nipple discharge nipple pain recent change In size skin changes chest pain edema fainting irregular rate palpitations rapid rate other ______________ abdominal pain bloating diarrhea constipation heartburn nausea rectal bleeding vomiting other _____________ abnormal vaginal bleeding absence of menses discharge frequent urination incontinence painful intercourse painful menstruation painful urination pelvic pain urgency vaginal dryness vaginal itching excessive urination at night other ____________________ Genitourinary Musculoskeletal Neurologic Psychiatric Endocrine Blood and Lymph Other hearing loss nose night sweats bleeds ringing ears sinus pain runny nose back pain joint pain joint swelling muscle pain muscle weakness other _____________ ADD(attention deficit) dizziness fainting headaches numbness tingling tremors seizures other _____________ anxiety depression insomnia memory loss suicidal ideation feels safe @ home frequent crying appetite change cold intolerance excessive thirst excessive urination heat intolerance libido change other ______________ anemia blood clots easy bruising prolonged bleeding swollen nodes other ______________ other 9/1/14